Fallopian tube occlusion accounts for about 25 to 30 percent of infertility cases, according to Columbia Doctors. While fallopian tube surgery is often called on to correct the problem, depending on the severity of the blockage, those looking to achieve pregnancy may need to go a step further.
By understanding each type of occlusion and utilizing key diagnostic tools such as ultrasound, clinicians will be better primed on both diagnosing fallopian tube problems and when to suggest surgery, nonsurgical treatment or in vitro fertilization (IVF).
Types of Tubal Factor Infertility and Treatment
Whether a patient may need to consider fallopian tube surgery depends on the location and extent of tubal scarring, damage or occlusion:
- Proximal tubal blockage: A blockage near the uterus is typically the easiest to treat, with the best chances of the patient going on to conceive naturally. Proximal occlusion can be treated nonsurgically with tubal cannulation, in which the physician uses fluoroscopy or hysteroscopy to guide a catheter into the fallopian tube.
- Blockage in the middle section: Scarring or previous tubal ligation can cause a blockage midway through the tubes. Tubal reanastomosis may be able to repair the blocked section or remove the damaged portion of the tube and connect the two healthy ends. If the damage is more extensive, salpingectomy may be needed to remove the tube. If one tube remains open, the patient still has a chance of conceiving naturally.
- Distal tubal blockage: When the occlusion is far from the uterus or the tube is completely blocked, salpingectomy may be the best option. The patient may also opt to avoid surgery and choose to begin IVF. This may be the most effective option if they have a distal blockage or damage to both fallopian tubes.
According to the Journal of Clinical Medicine, various studies have found that anywhere from 12 percent to 51 percent of patients may be able to spontaneously conceive after tubal patency is restored. As natural conception may take longer, recommendations should always consider a patient's health, age and severity of tubal factor infertility.
Hydrosalpinx Can Complicate IVF
One common type of distal tubal occlusion is hydrosalpinx. Unlike other types of tubal disease that can be ignored if the patient chooses IVF, hydrosalpinx must be treated. Hydrosalpingeal fluid can leak into the uterus, damaging the embryo or washing it away. Women with hydrosalpinx have up to a 50 percent lower chance of pregnancy from IVF embryo transfer, according to a study published in Medicine.
Laparoscopic salpingectomy or tubal ligation are considered standard treatment for hydrosalpinx, but newer fallopian tube embolization techniques have shown positive outcomes for pregnancy during IVF.
Multiple studies have found that tubal embolization, in which microcoils are placed in the fallopian tube to block the flow of fluid into the uterine cavity, improves the rate of pregnancy for IVF and is safe and effective for the patient. This procedure can feasibly be performed in an outpatient setting.
Accurately Diagnosing Tubal Factor Infertility With Ultrasound
Assessing tubal patency is a critical component of any infertility work-up. Laparoscopy and hysterosalpingography (HSG) are frequently used to examine the fallopian tubes. However, these procedures are invasive and often painful. HSG also involves exposure to radiation, which lengthens the time before oocytes can be retrieved.
An alternative is 3D hysterosalpingo contrast sonography (HyCoSy), or hysterosalpingo foam sonography (HyFoSy). Dr. Michael Grynberg, director of reproductive medicine and fertility at Hôpital Antoine Béclère, recommends 3D ultrasound as a first option for a basic infertility work-up. This procedure allows the clinician to obtain a detailed view of the uterine cavity and fallopian tubes with less time and patient discomfort. The images are stored directly into the patient file when kept in-office, and it's not necessary to have a radiologist read the results.
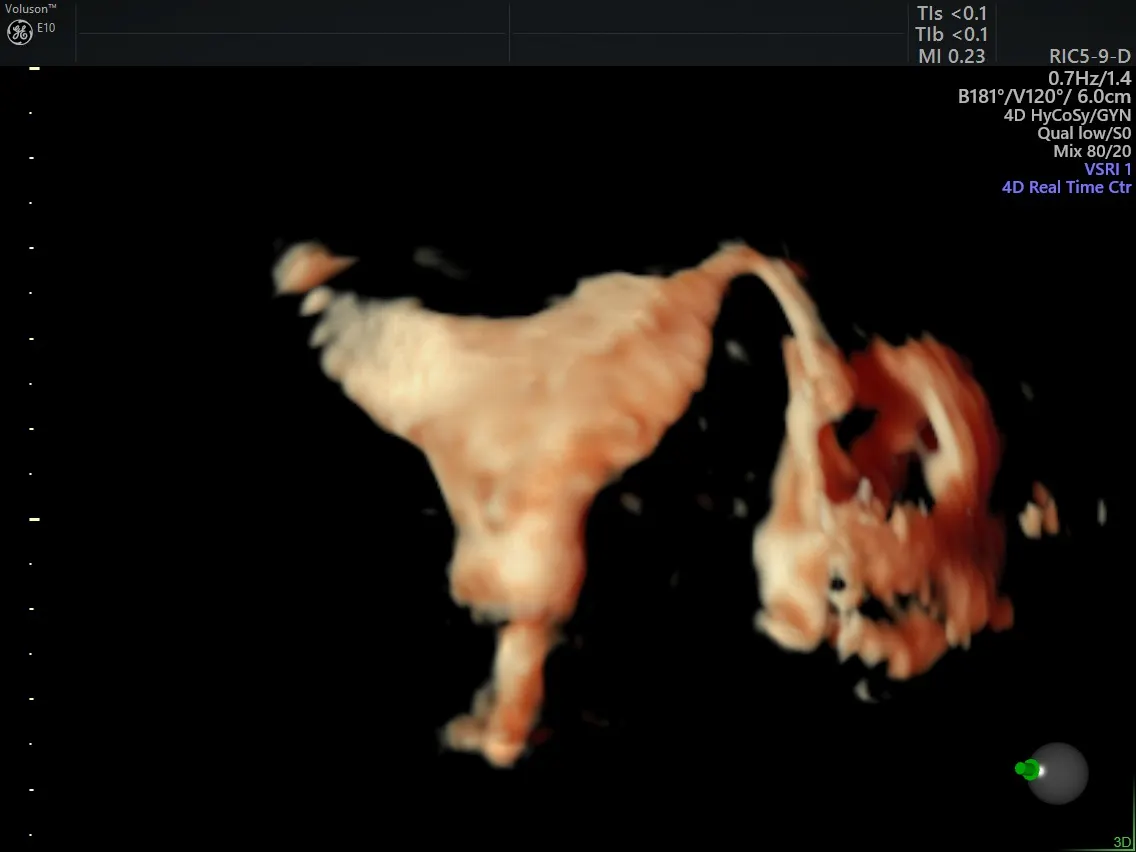
3D HyCoSy - Single Patent Fallopian Tube
3D HyCoSy: Single Patent Fallopian Tube
Learning to perform HyCoSy and HyFoSy can be intimidating at first, but Dr. Grynberg encourages physicians not to let that stop them.
"It's not hard to master the procedures, especially for physicians who have performed basic ultrasounds," he says. "Learning the technology should not be a drawback."
Ultrasound may continue to be used throughout the treatment of tubal occlusion to evaluate the effectiveness of interventions. A solid assessment and diagnosis allow patients to evaluate their options and choose the path that best suits their needs and preferences.