

It's common to hear phrases like, "It's that time of the month." Or, "Aunt Flo is here." On average, a woman will have 450 menstrual cycles in her lifetime. That equates to seven years of bleeding. If she experiences menstrual cramps for two or three days each cycle, that amounts to more than three years of cramps in a lifetime. The pain of severe primary and secondary dysmenorrhea can make those years feel like lost time.
Cramps that are painful enough to result in missed participation in educational, athletic and work opportunities can have severe consequences and impact a person's quality of life. It's time to remove the stigma surrounding menstrual cycles and demystify dysmenorrhea for your patients.
Menstrual Cramps Are Serious
Intense menstrual cramps are not normal. Instances of severe primary and secondary dysmenorrhea require evaluation if anti-inflammatories or hormonal treatment do not help, or if the pain lasts for more than a few days. Research on the subject tends to focus on younger women: American Family Physician reports that menstrual pain often reaches its peak during a person's late teens or early 20s.
The American Academy of Pediatrics reports that about half of adolescents who menstruate experience mild to moderate cramps, which typically last three to four days. About 15 percent experience severe symptoms, potentially from primary dysmenorrhea, resulting in school absenteeism.
Identifying Primary Dysmenorrhea
The American College of Obstetricians and Gynecologists (ACOG) defines primary dysmenorrhea as painful periods in the absence of pelvic pathology. High levels of prostaglandins in the endometrium cause uterine contractions; as the endometrium is shed, the level of prostaglandins decreases and cramps gradually diminish.
If a patient's history and evaluation suggest primary dysmenorrhea, treatment may include simple remedies, such as over-the-counter anti-inflammatories and continued, normal physical activity. Heat applied to the lower abdomen twice a day for 20 minutes may also alleviate pain. Prescribing oral contraceptives to suppress menstruation is considered safe. However, if the patient does not improve within three to six months, a targeted age-appropriate exam, lab work and ultrasound can help uncover other causes of painful menses.
Secondary Dysmenorrhea: Underlying Causes
Secondary dysmenorrhea is typically caused by a gynecologic disorder such as endometriosis, adenomyosis or fibroids or by congenital anomalies of the pelvic reproductive organs. This pain tends to escalate over time.
ACOG reports that approximately two-thirds of adolescents with chronic cramps who remain unresponsive to treatment are eventually diagnosed with endometriosis. Even if pelvic exam findings are normal, you should follow up with a pelvic ultrasound. Typical ultrasound findings for endometriosis — such as endometriomas, an obliterated cul-de-sac or a painful uterosacral nodule — may not be as obvious in a young patient who is in the earlier stages of the disease. While the conditions may be linked, there is a difference between endometriosis and dysmenorrhea. Laparoscopy is an option when the etiology of dysmenorrhea is uncertain.
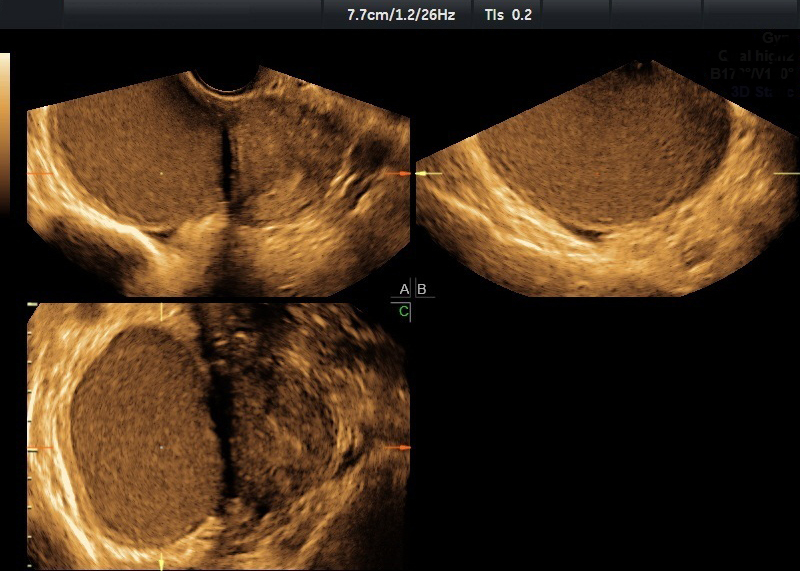
Typical appearance of an endometrioma on ultrasound
Clear and red vesicular implants of the peritoneum are more common in adolescents with endometriosis than the "powder burn" lesion typically seen in adults. These vesicular implants may be difficult for the inexperienced eye to identify. The symptoms may seem out of proportion to the surgical findings, but since these implants produce high levels of prostaglandin, even small lesions can cause significant inflammation and pain.
Primary and Secondary Dysmenorrhea Treatment
It is not always possible to confirm the pathology of dysmenorrhea with a small sample that may not survive processing — but you should attempt it nonetheless. Excising lesions is preferable to fulguration for preserving a patient's fertility.
Myths surrounding the true nature of menstrual pain are universal. Help your patients speak up and find treatment.

