

Uterine cancer is the most common gynecologic malignancy diagnosed in women in the developed world, according to the Centers for Disease Control and Prevention. Fortunately, most patients seek immediate care when they have abnormal uterine bleeding, and a simple in-office endometrial biopsy has proven to be highly sensitive in diagnosing or ruling out cancer.
However, diagnosing uterine cancer may not always be that simple. The patient may have cervical stenosis uterus concerns, for example, making biopsy difficult. Or your sample may be insufficient for diagnosis. The following wait for biopsy results can take weeks or longer.
To improve on this process, gynecologists should blend the art and science of medicine to strengthen the physician-patient partnership and gather information that can help guide the management of a uterine cancer diagnosis and minimize the patient's distress along the way.
Identifying Symptoms of Uterine Cancer
A thorough physical exam is a good place to start when diagnosing uterine cancer. Careful attention to the specific source of bleeding as well as to the potential for a larger uterine cancer bleeding pattern is a critical point in the stepwise evaluation. Even if no active bleeding is identified, conduct a 3D pelvic ultrasound to rule out gynecologic pathology. A blind biopsy without ultrasound is no longer the standard of care.
A point-of-care ultrasound should be as much a part of the physical as the bimanual exam itself. In the comfort of your office, a pelvic ultrasound will provide swift, comprehensive information. Imaging a thickened endometrium or hematometra, which is pathognomonic of endometrial cancer in postmenopausal women, will enable you to counsel your patient regarding next steps in an informed way.
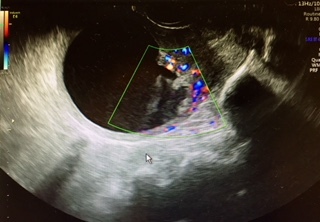
Ultrasound scan

Hematometra is pathognomonic of endometrial cancer.
Vaginal ultrasound of a uterus showing hematometra, which is associated with endometrial cancer (Images courtesy Dr. Lisbet Hanson)
Only about 15 percent of women seeking advice for postmenopausal bleeding have endometrial cancer, according to a study published in The Obstetrician & Gynaecologist. Another study published in the European Journal of Obstetrics & Gynecology estimated that the risk of endometrial cancer with an endometrium of 3 mm is 1 in 383. Sampling should be considered for anything greater than or equal to 4 mm.
In premenopausal women with abnormal uterine bleeding, the cutoff for endometrial thickness and sampling is not as clear. We know there is variation in the endometrium throughout the cycle, being thinnest during menstruation and thickest in the secretory half of the cycle. Many recommend endometrial sampling if the endometrium is thicker than 10 to 12 mm. In high-risk patients, such as those who are obese, have polycystic ovarian syndrome or Lynch Syndrome, or are on tamoxifen, sampling would not be criticized at any thickness.
Conducting a Stepwise, Evidence-Based Evaluation With Ultrasound
Remember to include an ultrasound exam of the ovaries when trying to diagnose uterine cancer. According to a study published in the Journal of Gynecologic Oncology, there is concomitant ovarian cancer in 5 percent of cases of uterine cancer. 3D imaging can make it easier to visualize pathology that might involve the adnexa and cervix. It is easy to do and the most cost-effective imaging tool available.
Exciting research by the International Endometrial Tumor Analysis Group is defining a vocabulary and helping to explain the ultrasound features of high-risk endometrial cancers. Since these have a worse prognosis than the more common adenocarcinoma of the uterus, identifying these types of high-risk tumors prior to surgical staging will help predict lymph node metastasis and the possible need for additional therapeutic intervention. Information such as the size of the lesion, echogenicity and color score will be valuable to help triage those patients who might benefit from additional preoperative imaging.
Whether postmenopausal or premenopausal, abnormal uterine bleeding calls for a stepwise, evidence-based evaluation of the female genital tract that includes a pelvic ultrasound and histologic evaluation of the endometrium. Survival depends on the stage at the time of diagnosis. While endometrial cancer typically occurs at the median age of 65, 25 percent are premenopausal at the time of diagnosis and 5 percent are women less than 40, according to a report published in the Journal of Obstetrics & Gynaecology of India.
Blending the Science of Medicine With the Art of Intuition
While science is analytic and rule-based, and provides decision models that can be applied to medical practice, the decisions themselves are lifeless without clinical judgment — the art of practicing medicine. A fusion of science, experience, intuition and pattern recognition comprises modern-day medicine.
Remember, interactive communication with your patients is crucial. Inform, involve, teach-back (have the patient repeat information back to you) and clarify with diagrams or models. This helps both auditory and visual learners understand and remember the information you want to convey. An informed patient is an empowered patient: Health literacy improves patient compliance, expectations and outcomes.
As William Osler, one of the founders of Johns Hopkins Hospital, said in the late 1800s, "The good physician treats the disease; the great physician treats the patient who has the disease." Who is the patient? What are her goals? How does her personal situation impact her treatment options? That is the practice of the art and science of medicine in gynecology so important to uterine cancer diagnoses.

