
Endometriosis is one of the most challenging gynecological pathologies to identify in a timely and accurate way. Many patients endure endometriosis pain for years due to the wide range of potential symptoms, incorrect diagnoses and elusive findings on imaging. However, with the advancement of imaging technology, endometriosis ultrasound examinations can now reveal more detail than ever before, allowing for more accurate identification of this subtle and complex pathology.
Endometriosis seen on Ultrasound
Is Endometriosis Visible on Ultrasound?
Part of the reason why patient symptoms can vary so widely is that endometriosis can occur in several different forms. Superficial endometriosis occurs when endometriotic lesions develop on the surface of peritoneal organs.
Endometriosis seen on ultrasound
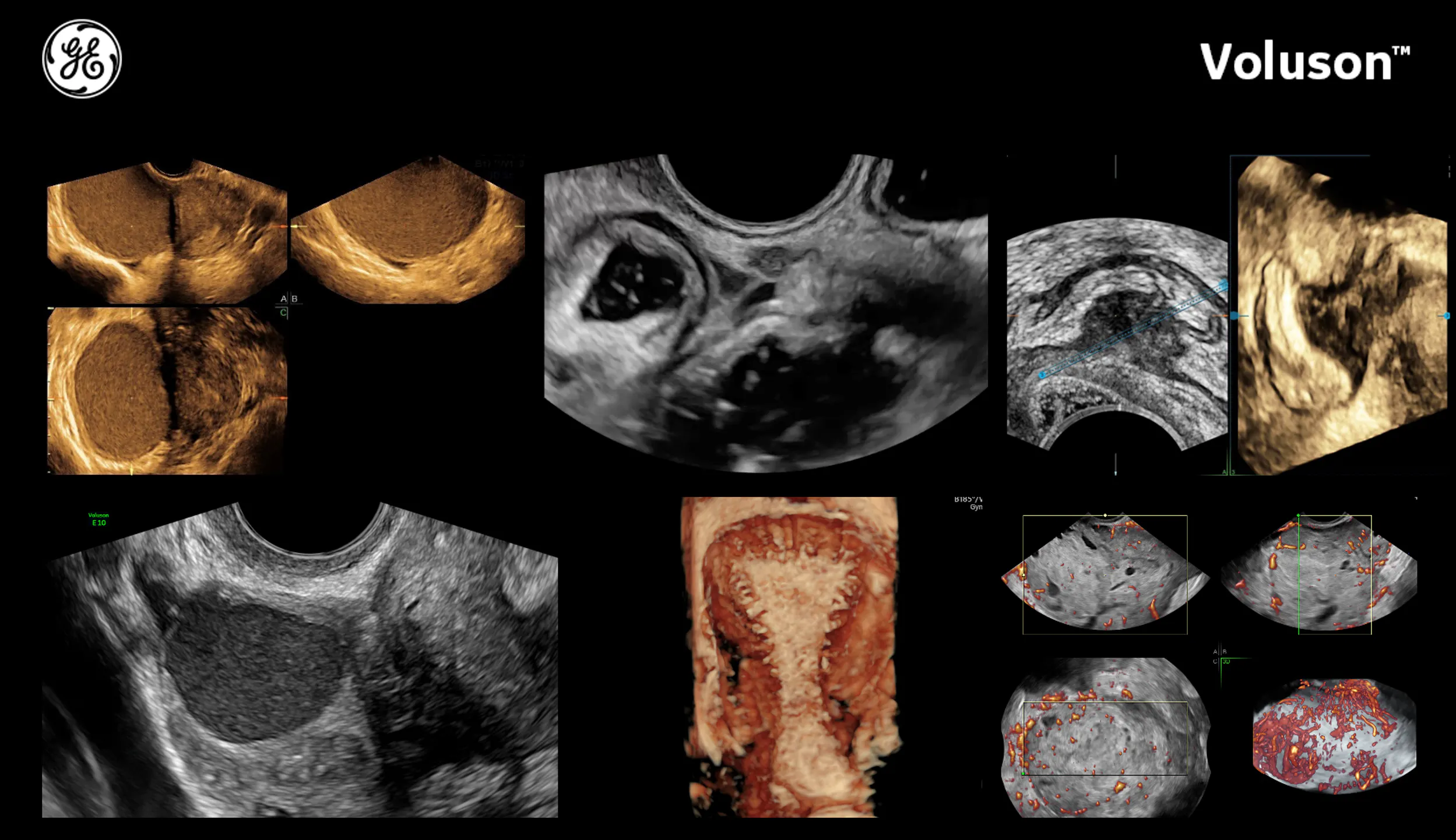
When endometriosis develops in the ovaries, it results in benign cysts filled with blood and fluid that are known as chocolate cysts (due to their brown color) or ovarian endometriomas. These two types are typically the easiest to locate and treat.

2D ovarian endometrioma
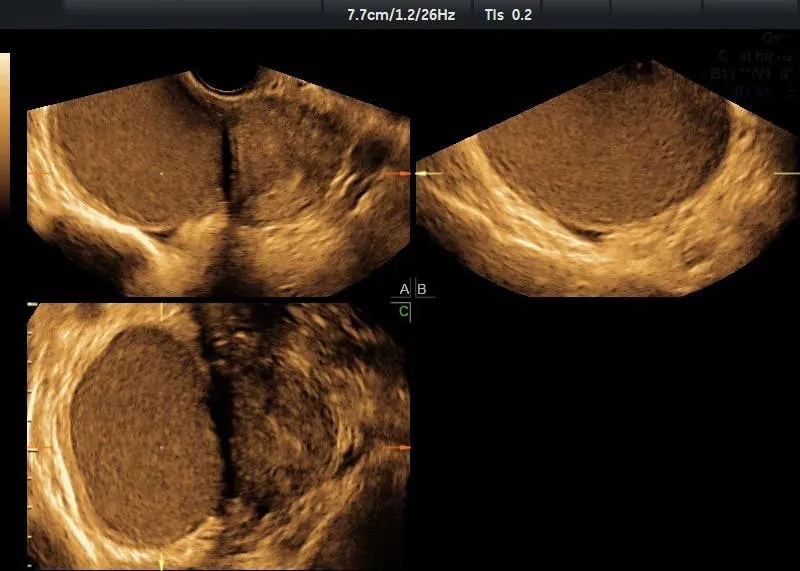
Typical 'ground glass' appearance of endometrioma as seen on ultrasound
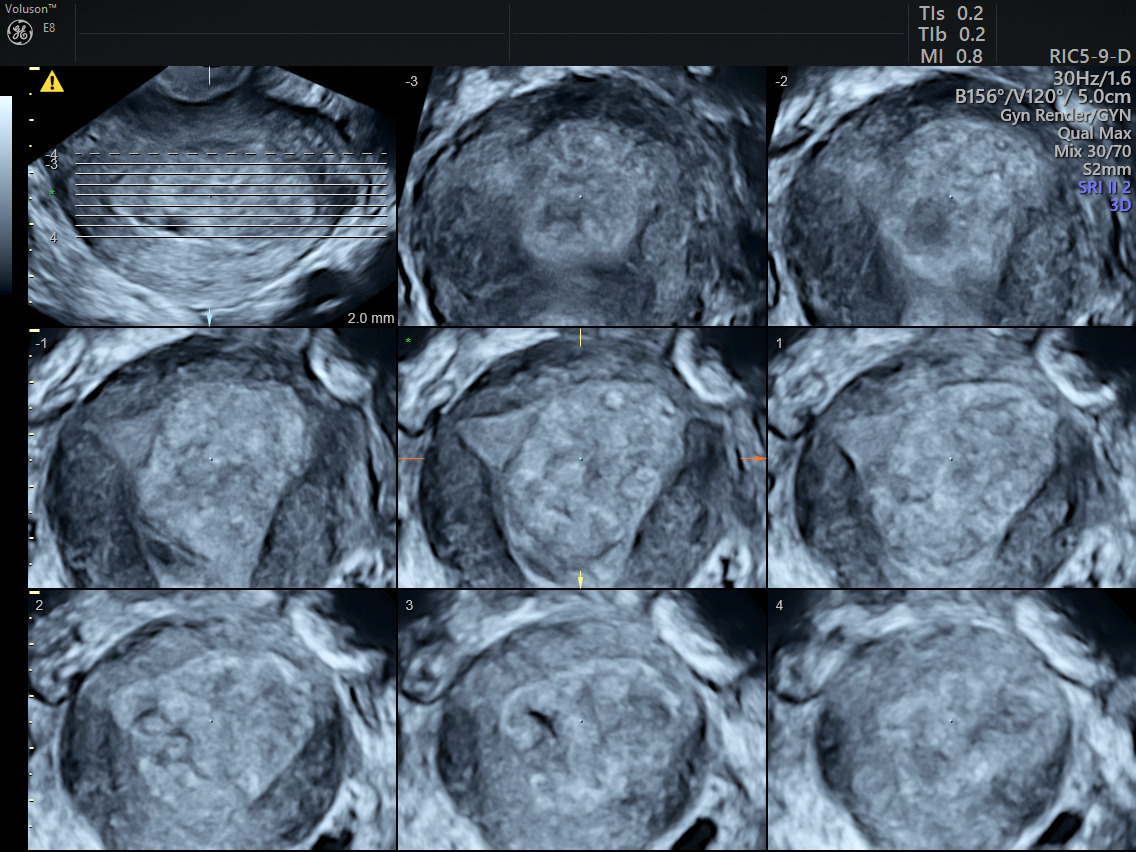
TUI endometrioma mass
The third form, known as deep infiltrating endometriosis (DIE), is more invasive than superficial or ovarian endometriosis. It occurs when endometrial tissue develops deep within other organs of the body. DIE can be found in a wide range of locations, such as the:
- Peritoneum
- Rectum
- Rectosigmoid colon
- Rectovaginal septum
- Vagina
- Uterosacral ligaments
- Urinary bladder
Determining the location of endometriosis spread is very important, as optimal treatment strategies are often site-specific.

Locating Deep Infiltrating Endometriosis
Laparoscopic surgery can be used to determine the location and extent of the disease. However, many patients prefer noninvasive imaging techniques. Having more than one option available gives patients more control over their health and treatment.
Transvaginal ultrasound and magnetic resonance imaging (MRI) are the most accurate ways to identify and assess the abdomen and pelvis for endometriosis. With its wide accessibility, low cost and ability to provide dynamic, detailed images, ultrasound is very widely accepted as a first-line imaging exam. Research has shown that transvaginal ultrasound examinations have a high sensitivity and specificity for the identifications of deep infiltrating endometriosis of the bowel when performed by experienced sonographers, according to research published in the International Journal of Women's Health.
It is also worth noting that many patients, especially those with more severe symptoms, prefer transvaginal ultrasound over MRI. For many, ultrasound is a more familiar exam that causes less anxiety.
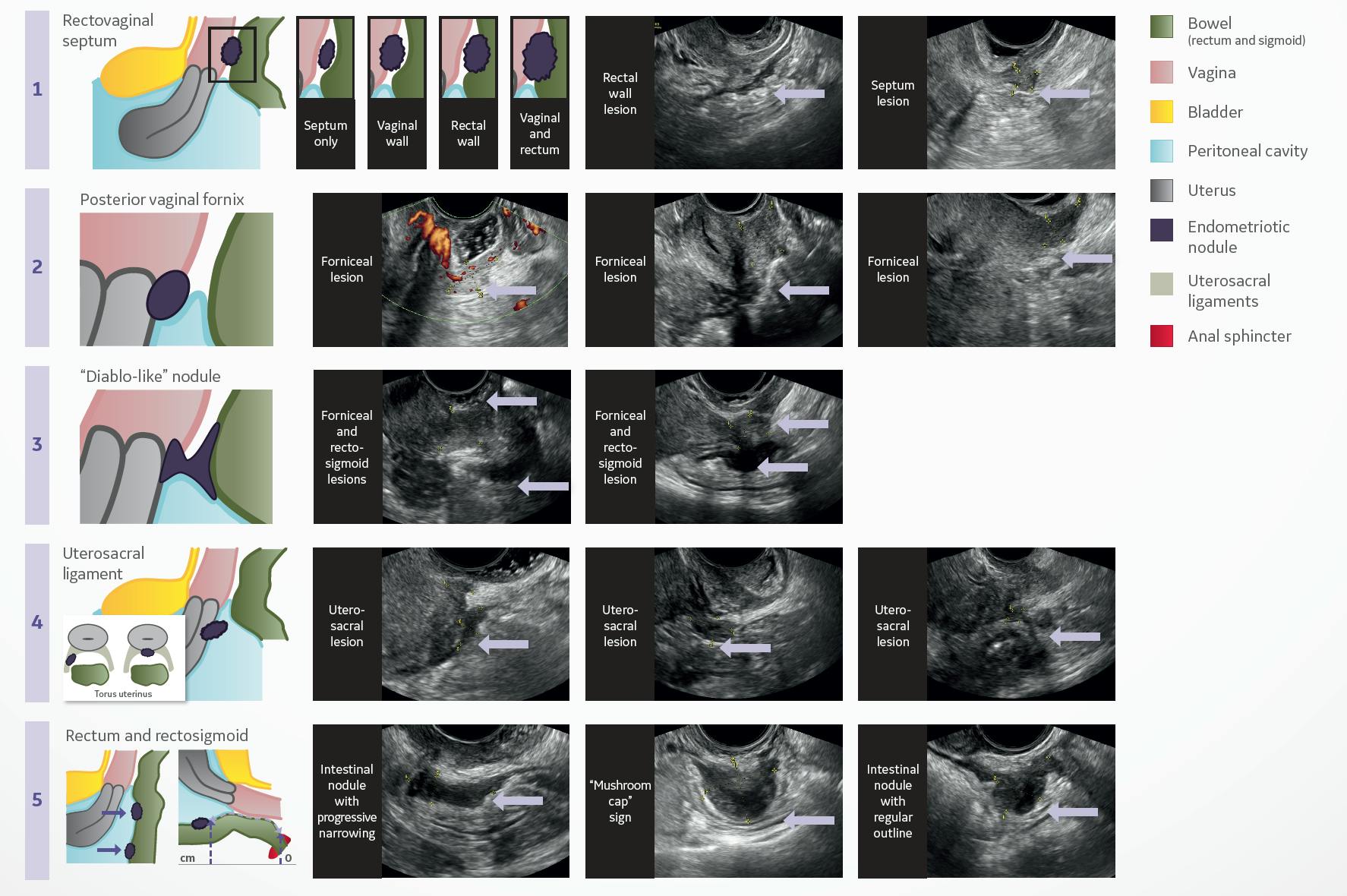
Deep Infiltrating Endometriosis Ultrasound Examinations
The rectum and rectosigmoid colon are two of the most frequently involved sites of bowel endometriosis, making up 70-88% of all cases, according to the International Journal of Women's Health study. Searching for DIE in the small intestine can be tricky for providers; bowel pain is easily mistaken for gastrointestinal disorders, which can lead to misdiagnosis, incorrect treatment and ongoing pain for patients.
Ultrasound offers clinicians an excellent assessment of the pelvis. Transvaginal ultrasound provides an even more detailed, close-up evaluation of areas of the pelvis. The most common areas of concern for DIE, the rectum and rectosigmoid colon, are very clear when viewed with transvaginal ultrasound.
Normal Bowel Appearance vs Bowel Endometriosis on Ultrasound
OB/GYNs should be able to recognize what a normal bowel looks like on ultrasound. Being able to clearly identify the normal bowel wall is a crucial first step in assessing endometriosis.
The bowel wall is composed of four layers and a central lumen. The outermost wall, the serosa, appears as a thin, echogenic line. Next is the muscularis, which is markedly hypoechoic. The third layer is the submucosa, which appears similar to the serosa—as a thin, echogenic line. These three layers are most commonly affected by deep infiltrating endometriosis.
The fourth and very innermost layer is the mucosa, which appears as a thicker hypoechoic band. The lumen of the bowel is usually echogenic in appearance, containing either fecal matter or air. Taken all together, the bowel wall appears as a series of alternating dark (hypoechoic) and light (echogenic) bands with a linear appearance.
The nodules of deep infiltrating endometriosis tissue typically develop from the outer serosal layer of the bowel wall, inward through the muscularis layer and sometimes even deeper into the submucosal layer. However, they only very rarely involve the innermost mucosa layer.
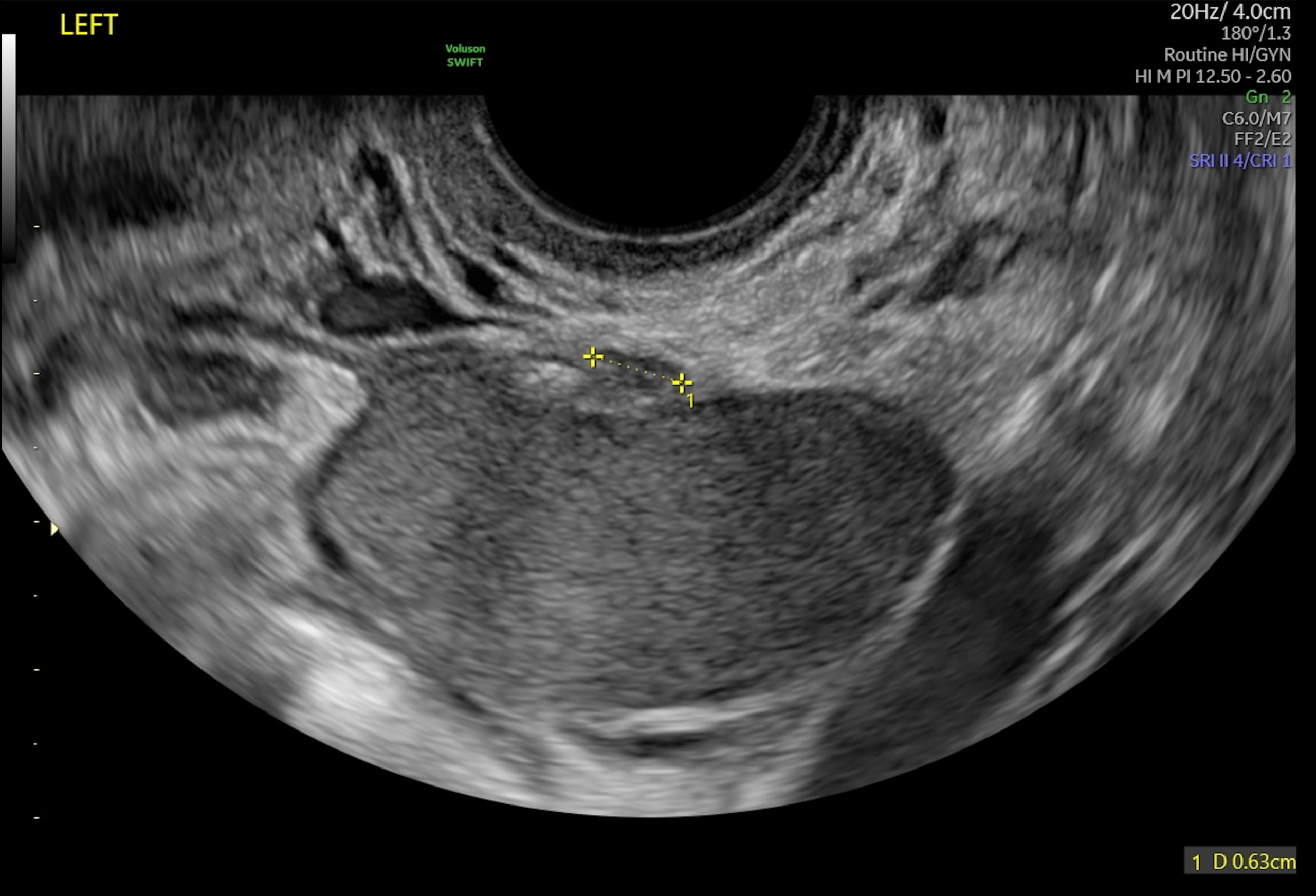
On ultrasound, deep infiltrating endometriosis will appear as hypoechoic irregular thickening of the bowel wall in a nodular or linear fashion. Assessment with color Doppler may reveal a few vessels coursing into the bowel wall.
When a lesion or area of concern is located, it should be imaging in both the long and short axis as well as measured in three dimensions: the length, width and anterior-posterior dimension. If possible, determine the distance of the lesion from the anal verge.
If one lesion appears, sonographers should continue to scan to ascertain whether there are multiple lesions present, as this can determine the preoperative risk of complications for the patient. The above-mentioned study published in the International Journal of Women's Health notes that when additional lesions are identified within 2 centimeters of the main lesion or are found to be affecting the same segment of bowel, they are classified as multifocal lesions. Lesions that are identified greater than 2 cm from the main lesion are classified as multicentric lesions.
Magnetic Resonance Imaging vs Ultrasound
While magnetic resonance imaging and transvaginal sonography can both help clinicians look for signs of deep infiltrating endometriosis, MRI is often less accessible for many patients due to both the expense and the availability of MRI machines in local clinics. MRI exams ultimately tend to have longer waitlists, which can extend patients' suffering while they wait for assessment, diagnosis and treatment.
One more efficient option is to perform a transabdominal and transvaginal ultrasound assessment first and then follow up with MRI if needed. This provides a faster path to diagnosis and treatment for patients suffering from endometriosis symptoms.
Historically, endometriosis has been managed surgically, by excising the nodules. The introduction of laparoscopic surgery has been of great benefit to patients. However, a growing number of endometriosis cases are managed with alternatives such as medication.
Ultrasound plays a large part in the accurate imaging, diagnosis and treatment of patients with all forms of endometriosis. A transvaginal ultrasound performed by an experienced technologist, along with a pelvic examination by an experienced clinician, can greatly improve the accuracy of endometriosis screening, diagnosis, monitoring and treatment.