
As the gynecology field moves toward more conservative approaches to ovarian pathologies, clinicians are becoming less inclined to consider oophorectomy, whether unilateral or bilateral. In fact, the number of oophorectomies performed in the United States has been waning steadily since 2005.
Still, unilateral oophorectomy is a medically appropriate choice for some conditions. In those situations, providers have wondered to what extent — if any — a unilateral oophorectomy affects a patient's overall fertility, and their chances of getting pregnant and carrying to term with IVF or other forms of assisted reproductive technology (ART).
Conditions That Indicate Oophorectomy
Whether oophorectomy is indicated depends on the circumstances of the patient and the disease. Performed either laparoscopically, vaginally or via laparotomy, the procedure may be recommended as a preventive or interventional measure for conditions such as:
- Cysts
- Endometriosis
- Ovarian torsion
- Pelvic inflammatory disease or tubo-ovarian abscesses
Oophorectomy is also sometimes offered as an elective procedure for women who have a high risk of ovarian cancer. It may be completed during a scheduled hysterectomy or as a stand-alone procedure.
Comparing Reproductive Outcomes Post-Oophorectomy
To better understand the potential effects of oophorectomy on ART, a meta-analysis published in BJOG assessed 21 retrospective studies spanning more than 30 years that compared IVF results from a total of 19,217 women, 1,045 of whom had a single ovary. The authors found that the absence of a second ovary impacted the quantity of the ovarian pool, but not necessarily the quality.
Participants who had undergone oophorectomy were found to have less ideal conditions for IVF success, measured by higher basal follicle-stimulating hormone (FSH) levels and lower serum E2 levels. However, the proportion of participants who became pregnant was about the same for women with one ovary versus two. The researchers did caution clinicians not to apply the conclusions to clinical practice since the studies were all retrospective.
The research on how a single ovary affects live birth rates is mixed. In a large-scale retrospective study published in Human Reproduction in 2018, researchers compared the live birth rates after IVF of 154 women post-oophorectomy with 22,693 women who had both ovaries intact. They found significant reductions in live birth rates for patients with a single ovary. However, those insights differed from previous studies that implied oophorectomy did not impact ART outcomes to a substantial degree.
After it was published, the large-cohort study stirred up a lot of outside reactions, including a letter to the editor that emphasized the study was inherently biased because it was retrospective in nature. That letter provoked a published reply reaffirming the results, limitations and all.
What This Means for Practitioners
A more conservative surgical approach should be considered when possible, in alignment with ACOG's recommendations, but individualized fertility planning will always be desirable for patients.
In order to assess ovarian reserve using ultrasound and obtain a precise antral follicle count, clinicians should use advanced ultrasound tools such as SonoAVCantral. This software automatically segments follicles within a volume. This reduces the risk of errors, which in turn reduces inter- and intraobserver variability and improves efficiency.
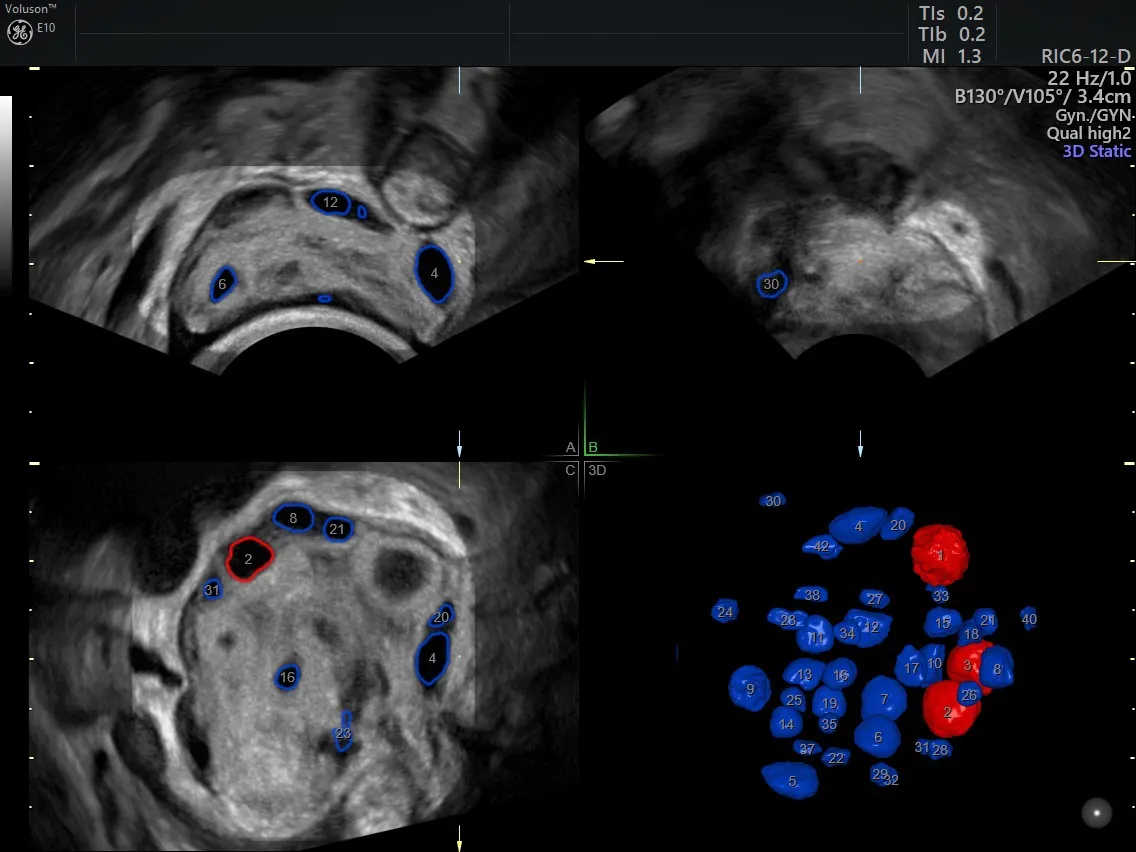
Ovarian reserve using Voluson™ SonoAVC™antral
Women can go on to have healthy full-term pregnancies after a unilateral oophorectomy, but their fertility route may require more planning and monitoring.

