According to data released by the Society for Assisted Reproductive Technology, more than 72,000 babies were born in 2017 as a result of IVF or other forms of ART. While fertility clinicians are experts in the technology and procedures that help patients build their families, not all of them are prepared to confirm a healthy pregnancy once a patient achieves one.
To confirm a clinical pregnancy following ART, reproductive endocrinologists must perform two evaluations: a blood test and a pregnancy confirmation exam using transvaginal ultrasound.
Blood Testing and Ultrasound: Two Key Steps for Pregnancy Confirmation
While fertility clinics vary in practice, most start by testing a patient's blood two or more times for human chorionic gonadotropin (hCG) approximately nine to 12 days after an embryo transfer, or 14 to 17 days after an insemination. The hCG number should double every 48 to 72 hours, according to Patient Management in Obstetrics and Gynecology. Although growth may be detectable earlier, some type of development should be seen on transvaginal ultrasound when hCG levels reach 2,000 mIU/ml, notes the American Pregnancy Association. For transabdominal ultrasound, the threshold is 3,600 mlU/ml.
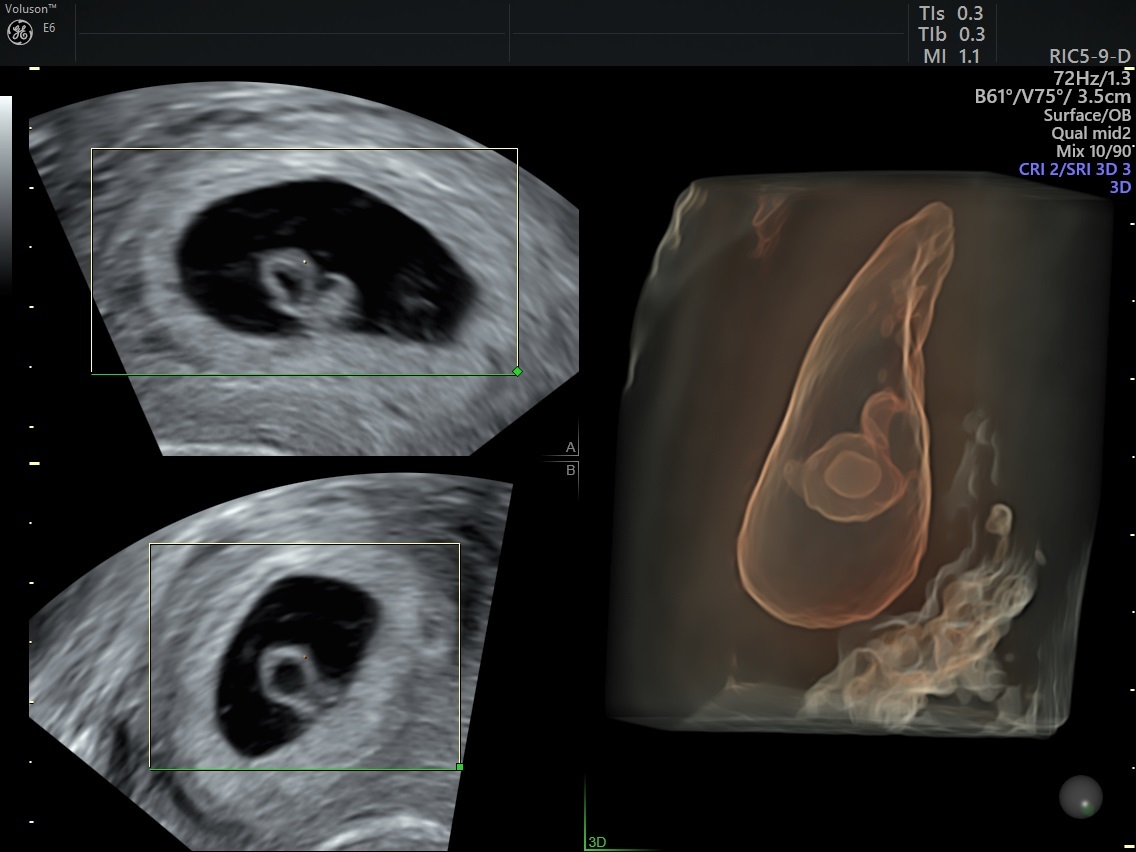
3D Ultrasound Image at 6 Weeks showing Yolk Sac
Starting at around ten weeks gestation, physicians perform between one and three transvaginal ultrasounds before referring the patient to an obstetrician. The first ultrasound is the initial attempt at a pregnancy confirmation exam, during which a clinician aims to verify an intrauterine pregnancy and possibly identify whether the patient has multiple gestations. Subsequent ultrasounds measure early cardiac activity and viability.
Expected Visualization and Measurements
Practice guidelines from the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) dictate that during the first transvaginal ultrasound, physicians should expect to see the following:
- Intrauterine implantation: Although it is rare, especially for IVF patients, it is possible for the embryo to implant outside of the uterus, such as in the fallopian tubes. This is a dangerous situation that nearly always results in miscarriage or pregnancy termination.
- Gestational sac: A dark image surrounded by dual echogenic rings
- Yolk sac: A round, white ring. The size at 10 weeks should be around 6 mm or smaller, according to Twining's Textbook of Fetal Abnormalities
- Fetal pole: Tissue adjacent to the yolk sac that develops along the chorionic margin. At five weeks gestation, it is approximately 2 mm in length. Initially, it grows 1 to 2 mm per day. At approximately 6.5 weeks gestation, it is visible as a distinct structure with cardiac pulsations, reports Twining's Textbook of Fetal Abnormalities.
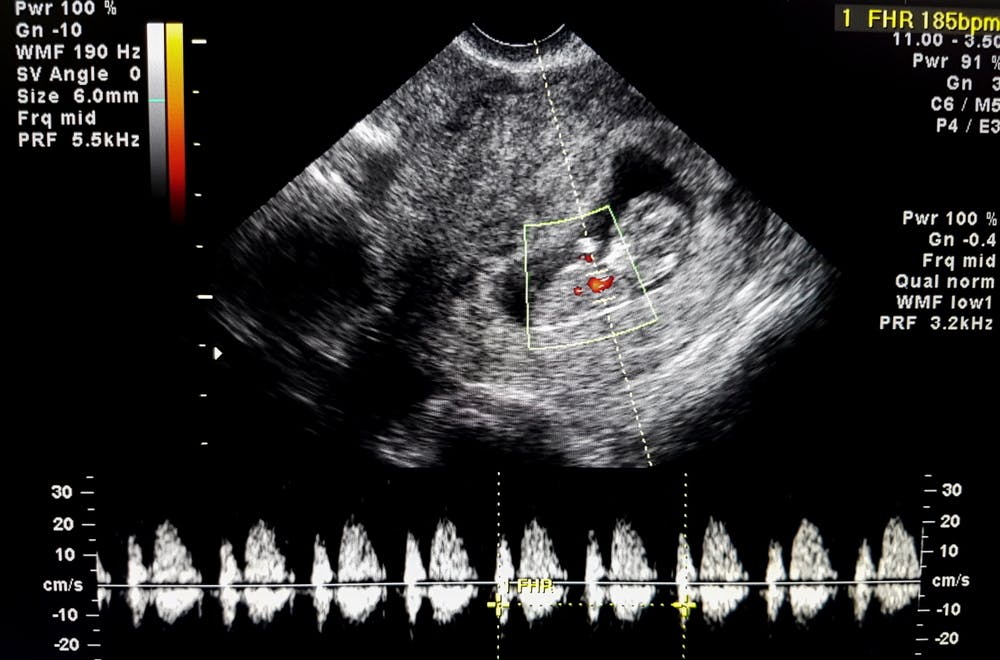
- Cardiac activity: If the length of the fetal pole is at least 5 mm, heart activity should be detectable. According to the American Pregnancy Association, the average heart rate at six weeks gestation is 90 to 110 beats per minute. This should increase over the next few ultrasounds.
Step-By-Step Pregnancy Confirmation Exam Guide
Step one: Evaluate the uterus, adnexa and cervix for the gestational sac.
If the gestational sac is seen, document the location. Even without cardiac activity, if the gestational sac is visualized in the uterus, it is considered an intrauterine pregnancy.
Examine the gestational sac for the absence or presence of a yolk sac and fetal pole. If possible, measure and record the crown-rump length (CRL), as this is the most accurate indicator of gestational age.
If it is very early in the pregnancy, instead of a yolk sac and fetal pole, eccentric intrauterine fluid collection with an echogenic rim will be visible. If there are no signs of an ectopic pregnancy, the fluid likely indicates an intrauterine pregnancy. However, follow up with hCG levels and a repeat transvaginal ultrasound to confirm.
Step two: Determine the absence or presence of cardiac activity.
Record any cardiac activity with a two-dimensional video clip or M-mode imaging, rather than pulsed Doppler ultrasound, to limit the rise in soft tissue thermal index. Typically, cardiac motion can be observed once the fetal pole is at least 2 mm. If the fetal pole is less than 7 mm but no cardiac activity is visible, repeat the transvaginal ultrasound in one week.
Step three: Document the number of gestations.
Chorionicity and amnionicity should be noted in the case of multiple gestations.
Step four: Evaluate the uterus, adnexa, cervix and cul-de-sac for abnormalities.
Image and document all abnormalities. Specifically, look for the presence, location, appearance, size and number of adnexal masses, leiomyomas, fluid and other uterine abnormalities.
When the Scan Is Abnormal
If the visualization or measurements are not as expected, it does not necessarily mean the pregnancy is nonviable. Some factors may lead to an incorrect diagnosis, such as:
- Variations in normal development: Especially early in a pregnancy, ultrasound findings may vary. If something appears abnormal, the best course of action is to repeat the ultrasound in one week.
- Differences in transmission: One patient's tissue might pass ultrasound waves differently than another. If the transmission is poor, the image may be unclear.
- Location of the gestational sac: If the gestational sac is too far away from the ultrasound probe, such as when the patient has a retroverted uterus, the image may be unclear.
Radiopaedia reports that if the gestational sac measures 8 mm with no visible yolk sac, or the gestational sac is larger than 16 to 24 mm but there is no fetal pole, then pregnancy failure is a distinct possibility.
International Differences
ISUOG recommends ultrasounds during the second trimester, but asserts that routine scanning during the first trimester (aside from an initial scan at 11 to 13 weeks) is unnecessary in the absence of a potential problem, especially before 10 weeks. This goes against some physicians' operational norms in North America, where some patients expect an ultrasound as early as six weeks gestation.
Meanwhile, the World Health Organization is trying to expand resources and training on offering a pregnancy confirmation exam to providers in poor and rural areas, who face more political, logistical and infrastructural challenges. International standards for correlating fetal CRL to gestational age do not exist.
Addressing Patient Fears
Especially in recent years, perhaps thanks to social media and pregnancy blogs, some pregnant patients fear that ultrasounds may harm their baby. However, according to the American College of Obstetricians and Gynecologists, "There is no evidence that ultrasound is harmful to a developing fetus."
Although patients cannot and should not be forced to undergo an ultrasound, providers should explain that a transvaginal ultrasound uses high frequency sound waves instead of radiation, making it safer than X-rays. Ultrasounds have been performed safely for decades, and are critical for identifying abnormalities that may lead to poor maternal or fetal outcomes.
Learning how to reliably confirm a pregnancy and ease patient concerns are crucial skills for any fertility clinician. Keeping abreast of international guidelines can help physicians address any gaps in their knowledge.

