
Ovarian hyperstimulation syndrome (OHSS) is a complication that can arise in some patients undergoing assisted reproductive treatments that require ovarian stimulation. According to guidelines published in Fertility and Sterility by the Practice Committee of the American Society for Reproductive Medicine (ASRM), moderate to severe ovarian hyperstimulation syndrome (OHSS) occurs in about 1 to 5 percent of IVF cycles.
The syndrome can be mild, moderate or severe, and the most serious form can become life-threatening. It is important for reproductive specialists to accurately identify at-risk patients and to monitor them throughout their fertility treatment.
What Are the Risk Factors for Ovarian Hyperstimulation Syndrome?
There are several independent risk factors for OHSS. These include polycystic ovarian syndrome (PCOS), an elevated response to gonadotropins and a previous history of OHSS, according to research published in the Journal of Human Reproductive Sciences. Young age and low body weight are two additional independent risk factors. Black women are also at a higher risk than Asian, Hispanic or white women for developing OHSS, according to research published in Fertility and Sterility. If a patient becomes pregnant while they have OHSS, the pregnancy can worsen the duration and severity of symptoms.
How Ultrasound Helps Detect OHSS
The key to preventing OHSS lies in careful monitoring of ovulation induction regimens though serial ultrasounds and frequent measurement of estrogen levels. Gonadotropins should be used at the minimum effective dose and duration.
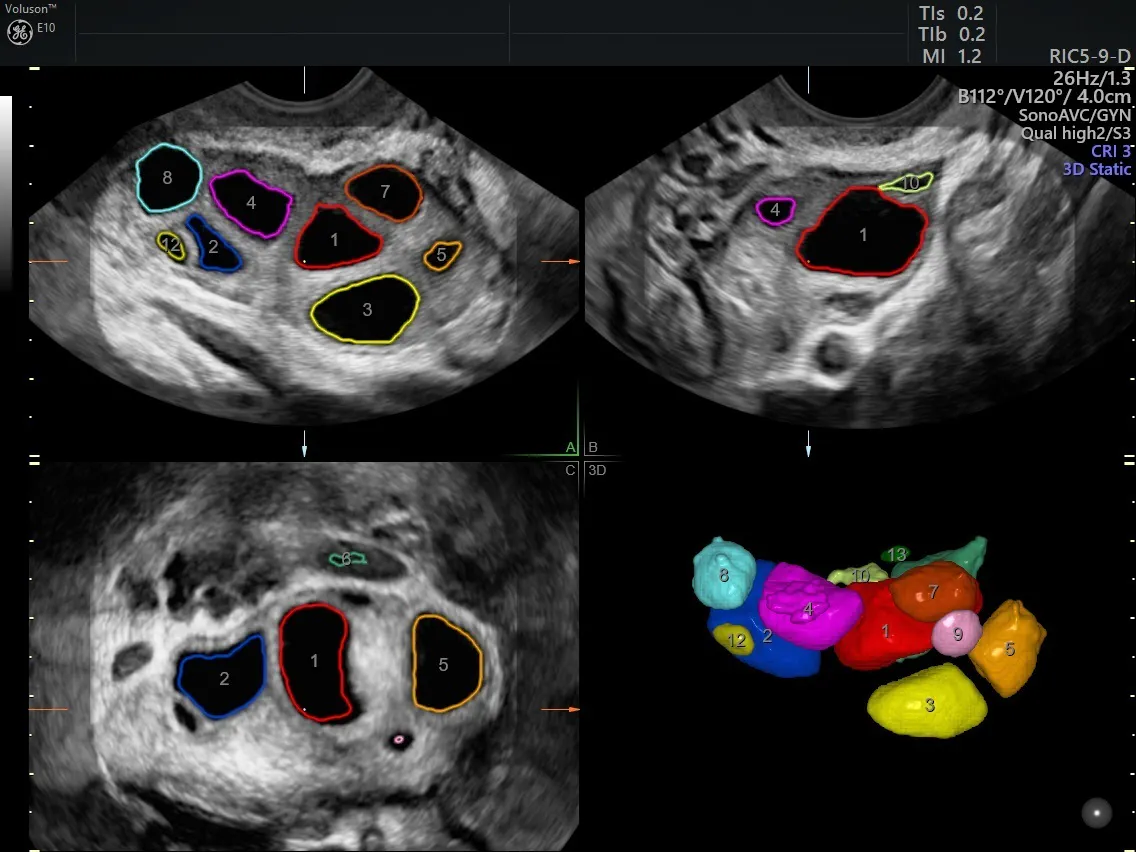
SonoAVC™follicle normal stimulated ovary
Monitoring specific markers in patients at high risk of the syndrome can help physicians to prevent it entirely, or to catch it early when symptoms are still mild and nonspecific. These markers include white blood cell (WBC) count, changes in ascites grade and maximum ovarian diameter (MOD). These parameters are measured during the early luteal phase after triggering final oocyte maturation with human chorionic gonadotropin, according to a study published in Ultrasound in Obstetrics and Gynecology. The researchers found that "the values of ascites grade, Ht [hematocrit] and WBC increased significantly" for all high-risk participants during a five-day observation window following oocyte retrieval.
In that same study, patients who developed severe early OHSS had increased MOD between day three and day five. Ovarian enlargement has previously been considered a marker of OHSS, and this study further supports the value of using ultrasound to measure ovarian diameter to monitor for the syndrome.
Clinicians should follow up-to-date clinical guidelines for ovarian stimulation, such as those published by the European Society for Human Reproduction and Embryology (ESHRE), to prevent OHSS as much as possible. Careful monitoring of specific markers via blood levels and ultrasound is an essential component of a successful ovarian stimulation regimen. OHSS tends to improve over seven to 10 days, according to the Royal College of Obstetricians and Gynaecologists; if a patient continues to worsen despite treatment, the physician should evaluate promptly for other possible issues.

