

Clinical thought leaders from around the globe — from North American to Australia — are encouraging women's health practitioners to obtain additional views following an initial routine gynecologic scan in women with chronic pelvic pain. Three additional steps are recommended, including looking for soft markers as well as dynamic, real-time ultrasound signs and carefully evaluating both the anterior and posterior pelvic compartments.
Combined, these four steps constitute a level 2 ultrasound exam. The goal is to identify endometriosis, the most common cause of chronic pelvic pain in women. The clinician should then map the extent of disease and plan appropriate therapy, whether medical or surgical, while educating the patient about the condition.
Diagnosing Chronic Pelvic Pain
While pelvic pain can be multifactorial in origin — including a variety of causes, from adnexal pathology and adhesive disease to interstitial cystitis and pudendal neuralgia — the single most common cause is endometriosis. Adolescents are not exempt from this lifelong and often debilitating disease.
Delay in diagnosis results in an average time to definitive diagnosis of eight years. The gold standard remains histologic confirmation of endometriosis. A carefully planned surgery by a clinician prepared to handle extensive disease is best realized with a careful exam and appropriate imaging prior to the very first incision.
Turning to transvaginal ultrasound for pelvic pain has been shown to detect endometriosis with high accuracy. While MRI also provides high sensitivity and specificity for the diagnosis of endometriosis, it requires a radiologist with interest in this disease process to interpret the results. In addition, the cost factor makes MRI prohibitive compared with ultrasound.
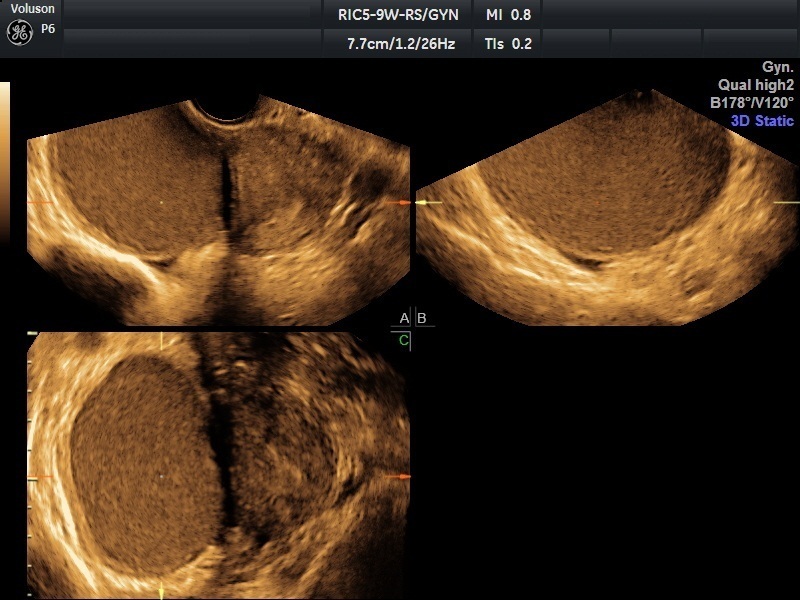
Level 2 ultrasound images of endometrioma; image courtesy of Prof Stefano Guerriero
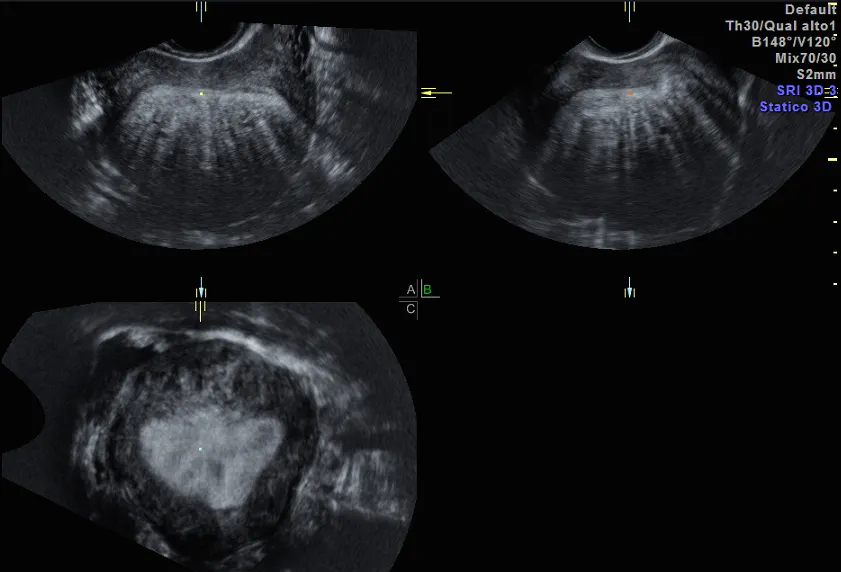
Level 2 ultrasound images of adenomyosis-fan shaped shadowing; image courtesy of Prof. Caterina Exacoustos
A 4-Step Process for Evaluating Endometriosis
Systematic protocols help minimize the omission of vital information that can aid the clinician in making an accurate diagnosis of pelvic pain. Standardized terminology and methods for identifying and measuring endometriosis are beneficial in research as well as clinical practice. A consensus opinion from the International Deep Endometriosis Analysis (IDEA) group in 2016 proposed a four-step evaluation for patients suspected of having endometriosis:
- Perform a standard ultrasound evaluation to look for adenomyosis and endometriomas.
- Look for soft markers, such as site-specific tenderness and ovarian mobility.
- Evaluate the pouch of Douglas (i.e. sliding sign) in real time.
- Look for deep infiltrating endometriosis (DIE) in the anterior and posterior compartment and beyond, including the bladder, ureters and rectosigmoid.
Some centers recommend separate fifth and sixth steps to look for evidence of hydroureter, which may require uretorolysis, and infiltrative nodules of the bowel, which may require discoid or segmental resection. In both instances, the patient has undergone a thorough evaluation. If the gynecologist diagnoses the patient with DIE or an obliterated pouch of Douglas, appropriate multidisciplinary surgical intervention may be the next step. This could potentially save the patient from inadequate or multiple surgeries for extensive or residual disease, avoiding unanticipated procedures and minimizing deleterious outcomes.
Practice Makes Perfect
Level 2 ultrasounds require some additional training and preparation. Videos, ultrasound courses and working with a trusted colleague can help you improve your technique and diagnostic accuracy. If you are comfortable with the first and second steps of the IDEA evaluation process, some additional practice will improve your ability to diagnose an obliterated pouch of Douglas. It is best to begin by focusing on the area of the rectocervix in interpreting results of the sliding sign.
Why not practice on routine transvaginal ultrasound exams as you begin adding this to your armamentarium of diagnostic tools? You can also begin identifying DIE nodules with sonovaginography. Instill approximately 20 to 50 cubic centimeters of gel in the anterior and posterior vaginal fornix to act as your acoustic window for inspection of the bladder base and rectovaginal septum.
Consider performing these procedures just before any planned diagnostic laparoscopy. Then, correlate your findings at surgery with those from the preoperative ultrasound. Your accuracy and confidence will improve over time, and you can begin to look further at the uterosacral ligaments, bladder and beyond.
Patient Care Is a Partnership
Consent is always a must. Don't forget to discuss what you are striving to accomplish with your patients. They will certainly appreciate your efforts on her behalf.
Chronic pelvic pain is a challenge to diagnose and manage. Level 2 ultrasound images can help you and the patient determine next steps and find the right treatment.



