

The presentation of uterine leiomyomas, or fibroids, is extremely variable. Some patients have no symptoms, but for the people who do, those symptoms can interfere with their quality of life. Depending on the size, shape and location of the fibroid, a patient may have heavy menstrual bleeding, back pain, pelvic pain, trouble urinating or unusually long periods. Fibroids can even affect fertility.
Many treatments exist for fibroids, and it takes a personalized approach to determine what is best for each patient. Invasive surgical treatments are some of the most effective and recommended, but many individuals do not want to undergo invasive surgery. In fact, research published in Obstetrics and Gynecology suggests that 25 percent of people with symptomatic uterine leiomyomas may put off treatment for up to five years. A relatively new FDA-approved technology — transcervical radiofrequency ablation — may be an option for patients looking for a nonsurgical option.
How Does Noninvasive Transcervical Radiofrequency Ablation Work?
Ultrasound-guided radiofrequency ablation has effectively reduced fibroids — and associated symptoms — for many patients for more than a decade. However, it can be a cumbersome procedure, using laparoscopic, transabdominal or transvaginal ultrasound to monitor the procedure and a separate tool to deliver the radiofrequency waves. The ablation may be done percutaneously or laparoscopically, so some patients still have an incision. Although the procedure has shorter recovery times than a hysterectomy or myomectomy, it still takes a few days to fully recover.
A recent FDA-approved technology has made the procedure easier by combining the ultrasound imaging device with the ablation device. This makes for a truly noninvasive procedure, performed transvaginally with no incisions.
To perform the procedure, a physician inserts the handpiece through the cervix to transmit a live ultrasound image. The physician finds the fibroid, and the device maps out an ablation zone that the clinician confirms. Then, the same device delivers the radiofrequency waves directly to the fibroid, using heat to shrink it. Ultrasound is used to monitor the fibroid and surrounding tissue throughout the procedure. The tailored ablation zone reduces the risk of damage to surrounding uterine tissue, nerves and blood vessels. No tissue is cut or removed during the procedure.
The same Obstetrics and Gynecology study that discussed patients putting off treatment, which was a prospective trial of ultrasound-guided transcervical ablation for fibroids, found that symptoms lessened for more than 96 percent of participants at 12 months. Trial participants experienced less menstrual bleeding and a reduction in fibroid size. Many had drastically reduced fibroid volume within four months.
How to Choose the Right Patients for Fibroid Ablation
The first step is to identify all fibroids through ultrasound screening. Transvaginal ultrasound is the first line of defense to detect and define uterine leiomyomas. They appear on ultrasound as solid, hypoechoic masses with a variable amount of acoustic shadowing. Ultrasound also allows the physician to look for potential complications, such as pelvic inflammatory disease or endometriosis, for which ablation may not be the best procedure.
Transcervical ablation is effective for most types of nonpedunculated fibroids, including submucosal, transmural, subserosal and intramural fibroids. The procedure may be an option for patients who adamantly wish to avoid surgery or removal of the uterus. It is also an option for those who are unwilling or unable to undergo hysteroscopic myomectomy.
Many patients are diagnosed with fibroids during their childbearing years; conserving fertility may be a big concern. It is important to discuss future pregnancy plans with each patient and discuss the risks and benefits of each procedure. Most clinical studies exclude patients who desire future pregnancy because of ethical reasons, so no definitive statements can be made about transcervical ablation and fertility preservation. Myomectomy remains the most recommended option for those who wish to become pregnant in the future.
However, research has reported cases of individuals who have had healthy pregnancies after radiofrequency ablation. A review published in the Journal of Minimally Invasive Gynecology found a total of 20 pregnancies across the literature after radiofrequency ablation of uterine fibroids. One of these pregnancies resulted in a spontaneous abortion, seven were electively terminated and 12 resulted in full-term live births. The number of reported pregnancies remains small, but the review noted that there have been no reported cases of abnormal placentation, uterine rupture or prematurity. One study published in the International Journal of Women's Health reported that two patients who have undergone transcervical ablation with the newer FDA-approved technology as part of a clinical trial have since had normal pregnancies with no complications.
Your patients should understand the reported outcomes, possible complications and limited information available on pregnancy and ablation before making a decision about the procedure.
Post-Procedure Care and Follow-up
The short recovery time is a big benefit for this same-day procedure. Patients do not need general anesthesia; about half of those in the trial returned to work within a day. All of them returned to normal activities within two days, a faster recovery time than most currently available treatment options for fibroids. The average facility stay for the procedure in the trial was 2.5 hours. No serious adverse events were reported.
Hysterectomy removes the possibility of uterine fibroids. All alternatives to hysterectomy may require surgical intervention at a later date to remove any new fibroids. Transcervical radiofrequency ablation has shown good long-term outcomes so far. In the clinical trial, 99 percent of patients did not require surgical reintervention at 12 months, which was the established follow-up period for the trial.
Transcervical radiofrequency ablation has broad applications for most fibroid types and may be a viable option for your patients. The noninvasive, uterine-sparing nature of the procedure, quick recovery times and low safety risks make it an appealing choice for symptomatic individuals who would otherwise delay treatment. Be sure to thoroughly discuss the details of the procedure and known outcomes with patients to help them decide the best treatment for uterine leiomyomas.
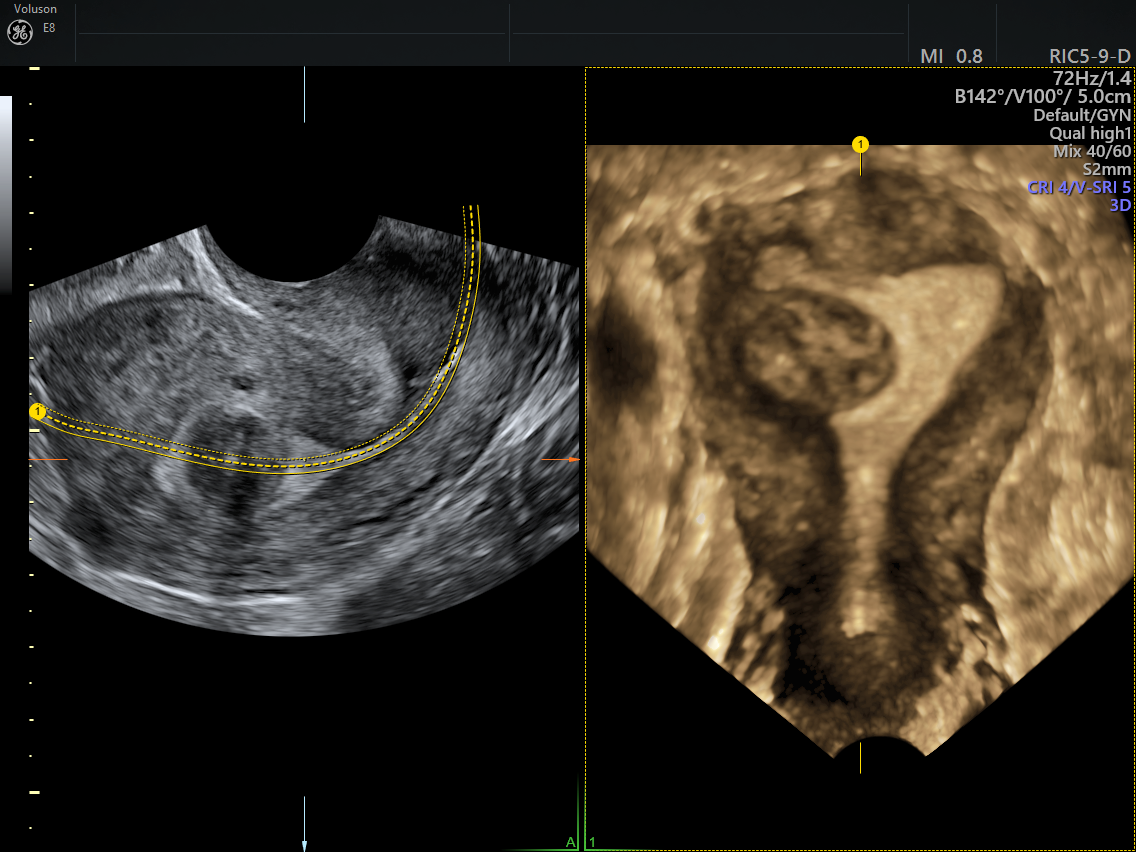
3D image of submucosal fibroid

