
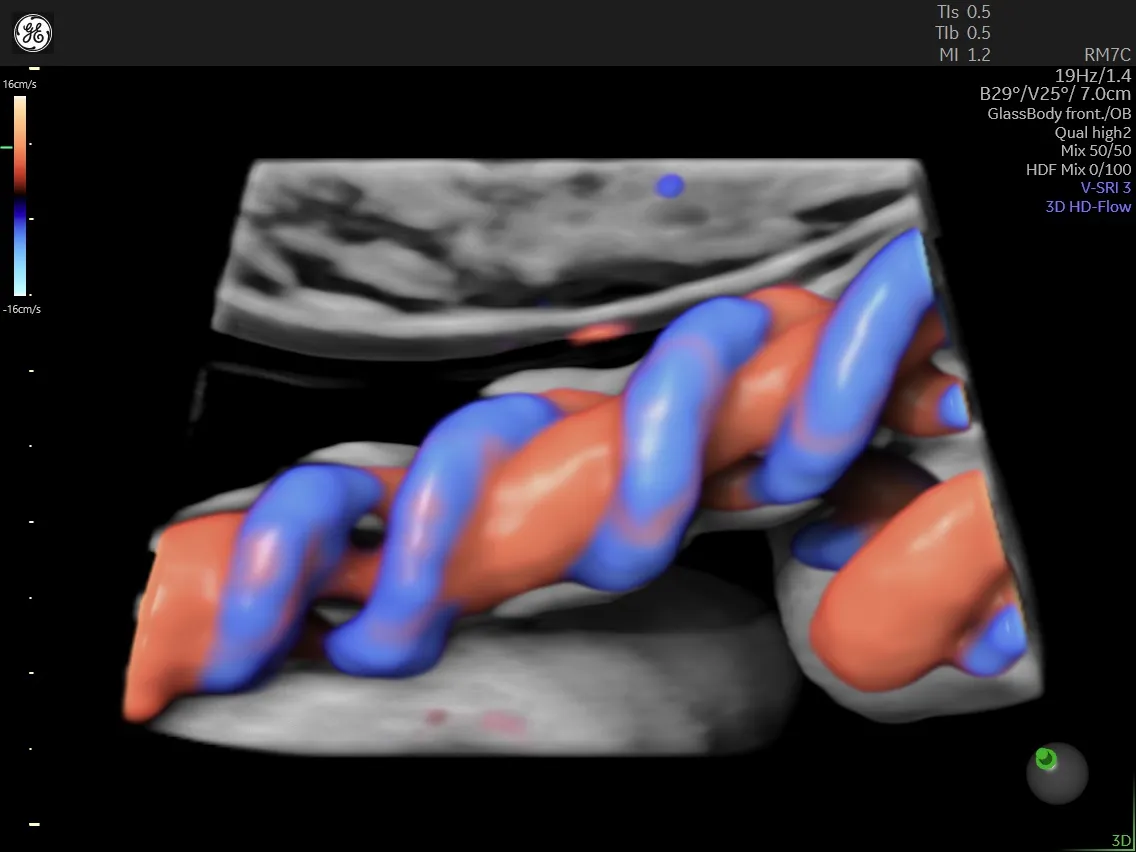
During pregnancy, the growing fetus is connected to the placenta by an umbilical cord. The umbilical cord is composed of one vein and two arteries. This umbilical vein carries nutrient-rich and oxygenated blood from the placenta into the fetal circulatory system. The smaller umbilical arteries are paired and carry deoxygenated blood out of the fetus into the placenta, pumped by the fetal heart.
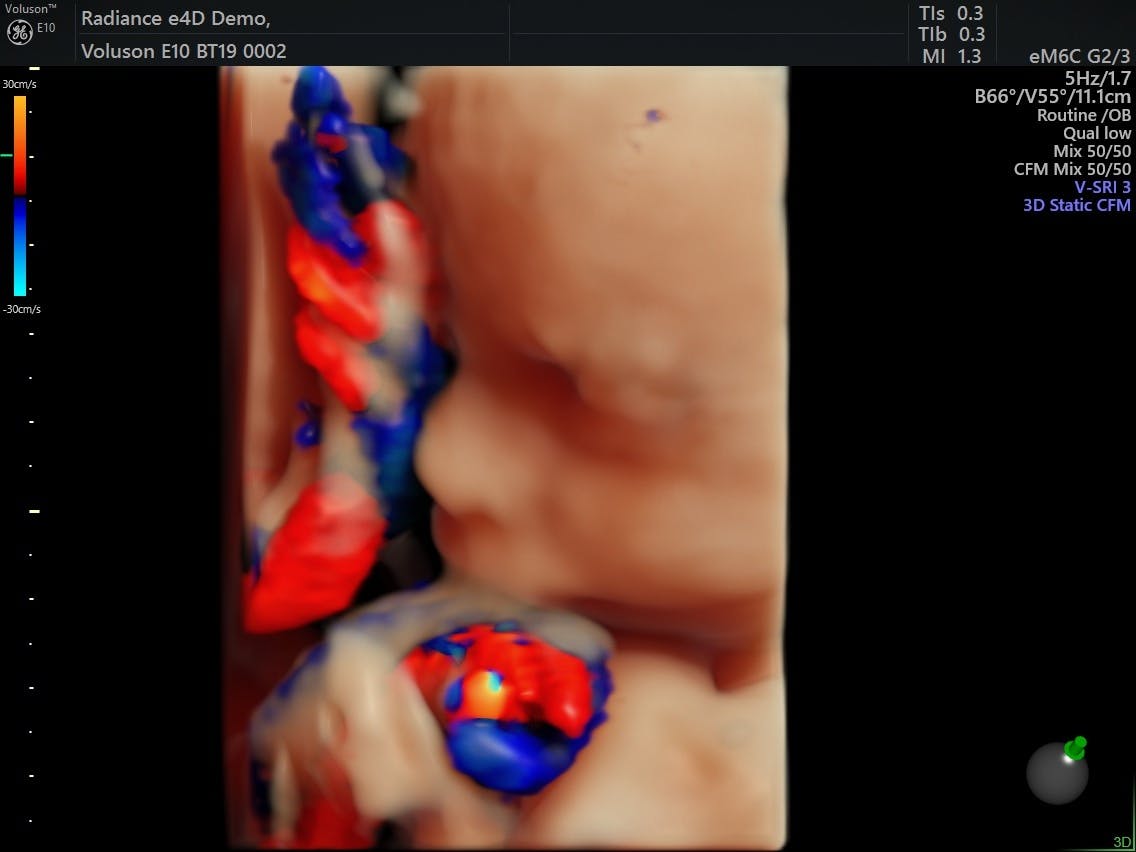
First-trimester fetus, Voluson™ HDlive™ imaging technology.
The umbilical cord of a fetus can be easily seen in the second and third trimesters and is routinely assessed. In addition, umbilical artery Doppler assessment can be done in both the second- and third-trimester ultrasound exams. This evaluation can provide information on fetal placental and cardiovascular function based on blood flow resistance. It is a non-invasive method of studying hemodynamic patterns to determine fetal well-being. This is especially important in any fetus with known or suspected intrauterine growth restriction (IUGR) or cord compression from a nuchal cord or knots.
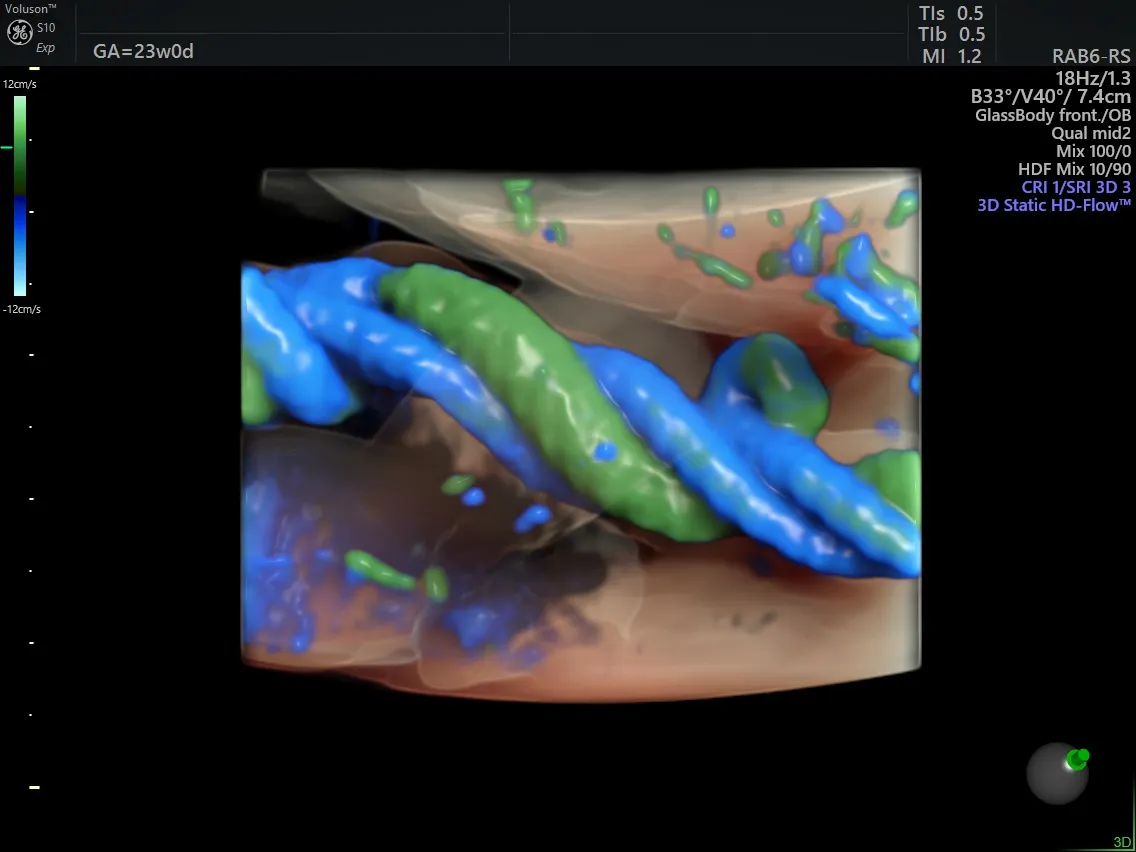
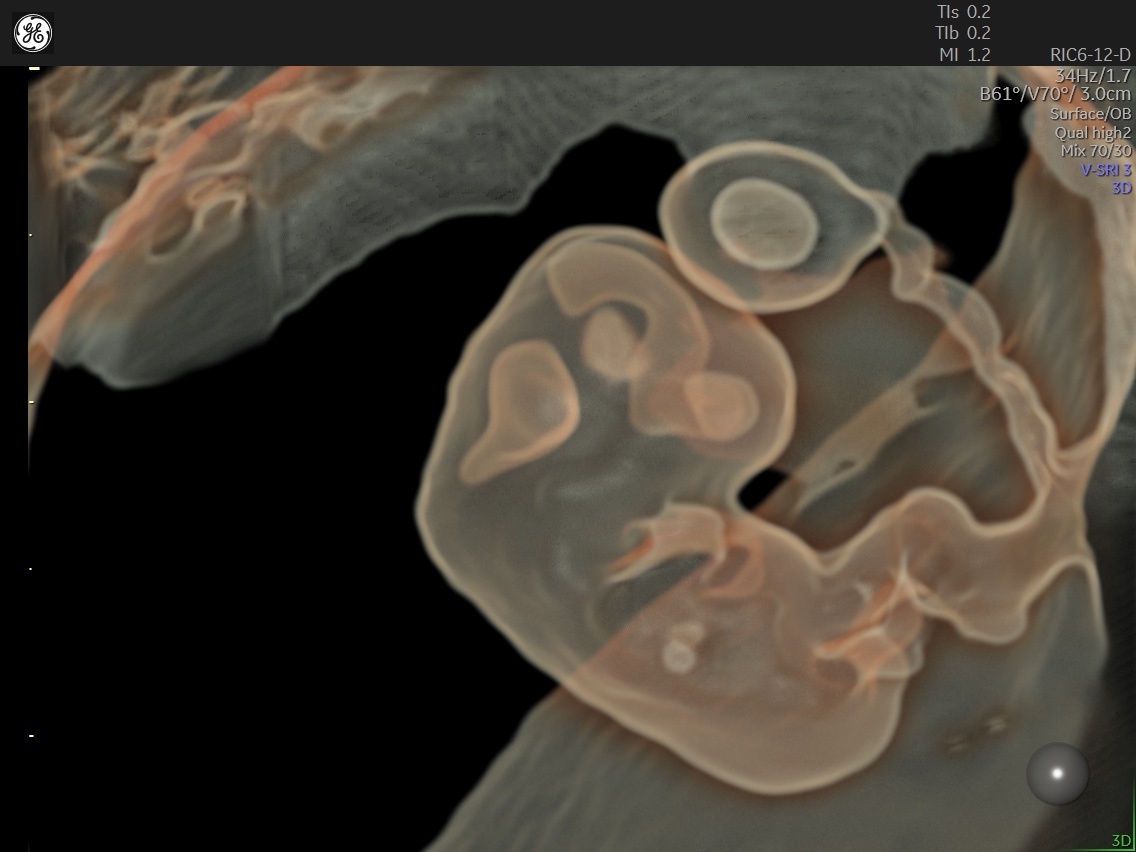
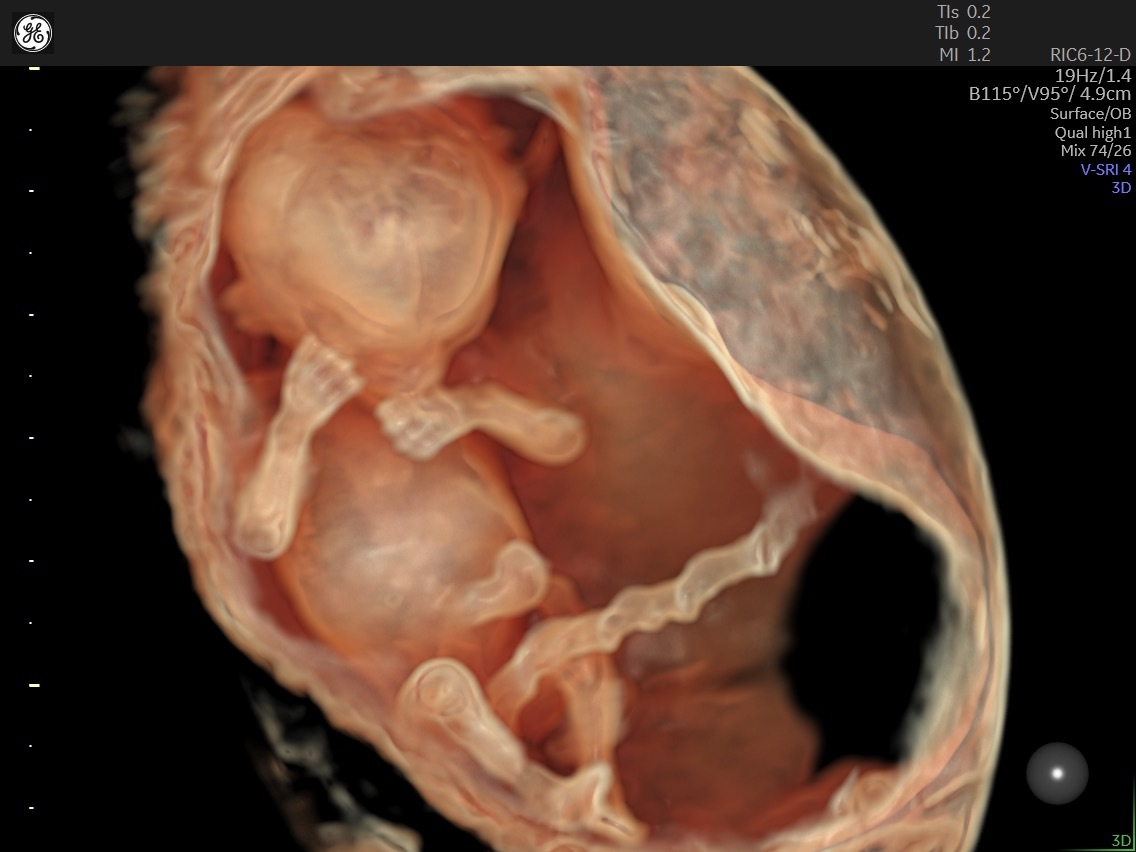
Umbilical cord using HDlive™ imaging technology.
How to Perform an Umbilical Artery Assessment
When it comes to umbilical artery Doppler assessment, the first thing to know is that blood flow through the umbilical artery can vary due to fetal heart rate, fetal movement, maternal breathing, and the location of the sampling site. For this reason, it is ideal to obtain Doppler tracings when the fetus is not active, and if needed, with suspended maternal breathing.
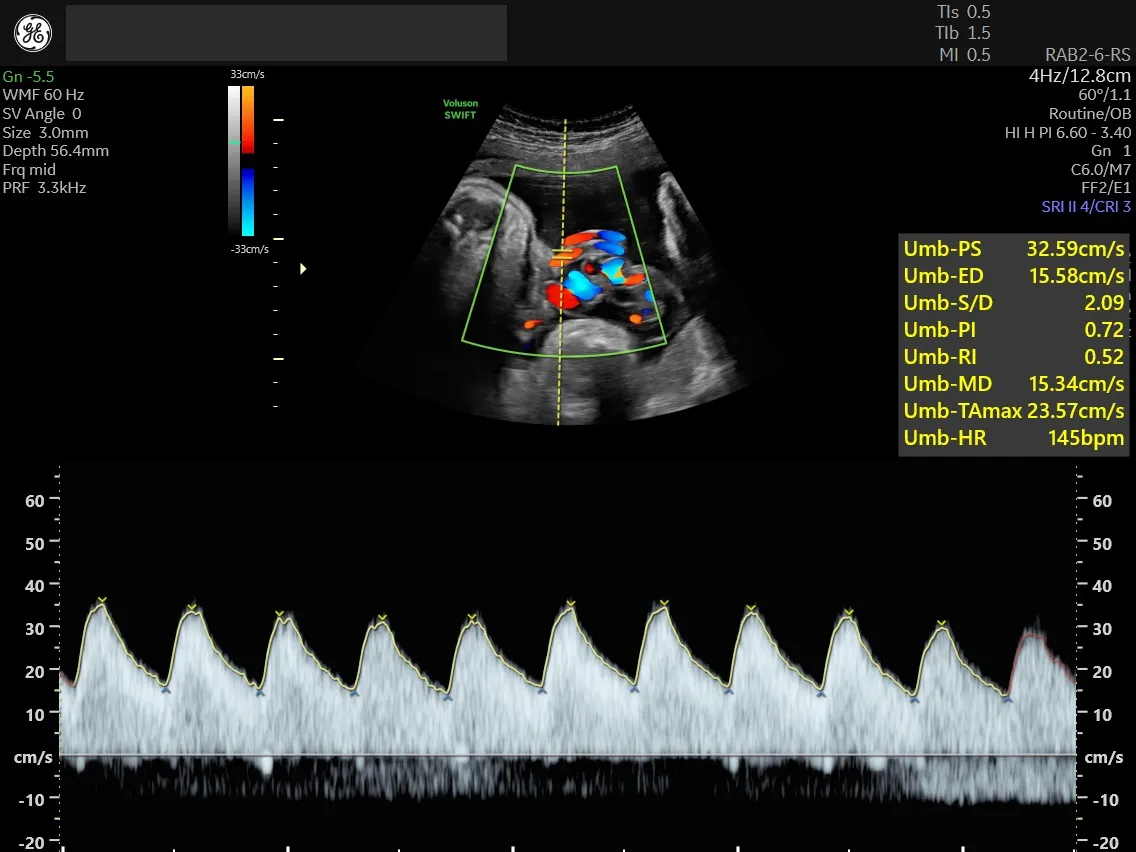
Pulse wave Doppler of 37-week fetus.
The optimal location to take Doppler readings is in a portion of free-floating cord, near either the placental or umbilical cord insertion sites. It is very important to maintain consistency of the sampling site, in addition to taking multiple measurements at the chosen site to allow for averaging of the final ratios. Averaging multiple samples, from the same location, minimizes the effect of the maternal and fetal physiological influence.
Some other factors to consider when undertaking an umbilical artery Doppler assessment are as follows: Sampling done closer to the umbilical insertion tends to have higher ratios due to lower end-diastolic flow compared to those obtained closer to the placental cord insertion. It is not necessary to obtain a specific degree of angle to the artery for the Doppler tracing as the angle is unknown. The resistive index (RI) and pulsatility index (PI) ratios are used instead to eliminate the need for angle-dependent Doppler. Venous flow tracing can also be easily obtained at the same time as arterial tracing. Simply increase the size of the Doppler gate to include both the artery and the vein in the color Doppler image.
Umbilical artery Doppler provides useful information about underlying increases in placental vascular resistance. This is measured using the following Doppler equations:
- RI: Peak systolic velocity – diastolic velocity/peak systolic velocity
- Systolic/Diastolic Ratio (S/D): Peak systolic velocity/diastolic velocity
- PI: Peak systolic velocity – diastolic velocity/mean velocity
Whichever ratio is used, the overall hemodynamic change assesses the increase in resistance within the umbilical artery. As a normal pregnancy progresses through the second and third trimesters, the resistance in the placenta — and, therefore, the umbilical arteries — will decrease. It is considered normal to see, via serial examinations of third-trimester ultrasound, Doppler measurements of resistance that either decrease or stay the same. It is abnormal to see any signs of increasing resistance, represented as stunted, absent, or retrograde diastolic flow, and the consequent increase in either PI or RI.
Normal Ratios and Resistance
A normal umbilical artery Doppler waveform has a low resistance pattern throughout gestation. The umbilical arteries are influenced by the rapid rate of the normal fetal heart — which, at 160–200 beats per minute, leads to a constant forward flow of blood toward the placenta, during both diastole and systole cycles of the heart.
In the second trimester and first half of the pregnancy, the umbilical artery will demonstrate minimal end-diastolic flow due to higher peripheral resistance in the placenta. At this age, the placenta is composed of fewer vessels, but vessels will increase as the pregnancy progresses into the third trimester. The S/D ratio in the second trimester is normally between 3.3 to 4.3 and will decrease to between 1.7 to 2.4 in the third trimester.
The International Society of Ultrasound in Obstetrics and Gynecology recommends that equipment used to perform Doppler studies of the umbilical cord include the following:
- Spectral and color Doppler flow capability with on-screen display of velocity scale and Doppler frequency display in MHz
- On-screen display of mechanical index and thermal index
- Display of the complete Doppler waveform
- System calculation of the peak systolic velocity, end-diastolic velocity, and time-averaged maximum velocity
- Calculation of commonly used Doppler indices (PI, RI, and S/D); tracings should be marked for calculation variables to allow for confirmation of correctly calculated values
Abnormal Umbilical Artery Doppler
In order to correctly interpret Doppler waveforms, care must be taken to note the flow direction in the arterial Doppler assessment. Reversal of the end-diastolic flow is worrisome for fetal mortality. Also, normal Doppler measurement ratio changes with gestational age, so the appropriate Doppler charts should be referenced for the gestational age of the fetus.
However, there are classic waveform appearances that are associated with negative fetal outcomes. The first sign of an abnormality is the loss of the end-diastolic component of the waveform, which results in a higher index number. This occurs because placental insufficiency is increasing. This increases the resistance in the vascular bed of the placenta, connected to the umbilical arteries. As that insufficiency progresses, the end-distolic component disappears and can even be reversed (appearing below the baseline in the Doppler tracing). In the case of advanced placental insufficiency, damage to the placenta can reach up to 75%. In these cases, the umbilical vein will also demonstrate abnormalities in flow reversals and pulsations.
When umbilical artery Doppler assessment is abnormal, it can be indicative of serious conditions, such as preeclampsia, pregnancy-induced hypertension, or fetal IUGRs. These conditions all require more vigilant obstetrical care and more frequent check-ins to assist in identifying the appropriate timing of fetal delivery for the best fetal and maternal outcomes.
Umbilical Artery Doppler in Twins
In a multiples pregnancy, Doppler tracings are obtained in the same manner as in a singleton pregnancy. Abnormal umbilical artery Doppler patterns in twins are associated with increased risk for pre-term delivery, low birth rate and neonatal morbidity.
Twin pregnancies with absent or reversed end-diastolic flow in the umbilical arteries experience higher incidences of growth discordance. There is also twice the incidence of twin-to-twin transfusion syndrome and perinatal morbidity.
The Single Umbilical Artery
The single umbilical artery occurs when only one of the paired umbilical arteries is present in the umbilical cord, along with the umbilical vein. This occurs in approximately 1% of singleton pregnancies and 3% of twin pregnancies. These pregnancies have associated fetal malformations in 17.6% of cases.
The most reliable technique to evaluate the number of vessels present within the umbilical cord is to assess the fetal pelvis with color or power Doppler — at the level of the bladder — to determine the number of arteries lateral to the bladder. In normal cases, where two umbilical arteries are present, there will be one artery present on each side of the bladder that joins together with the umbilical vein at the abdominal wall to form the normal umbilical cord. When only one artery is present alongside the bladder, this is documented as a single umbilical artery. A transverse view of a section of free-floating umbilical cord can also reveal either a two-vessel cord (one vein and one artery) or a three-vessel cord (one vein and two arteries).
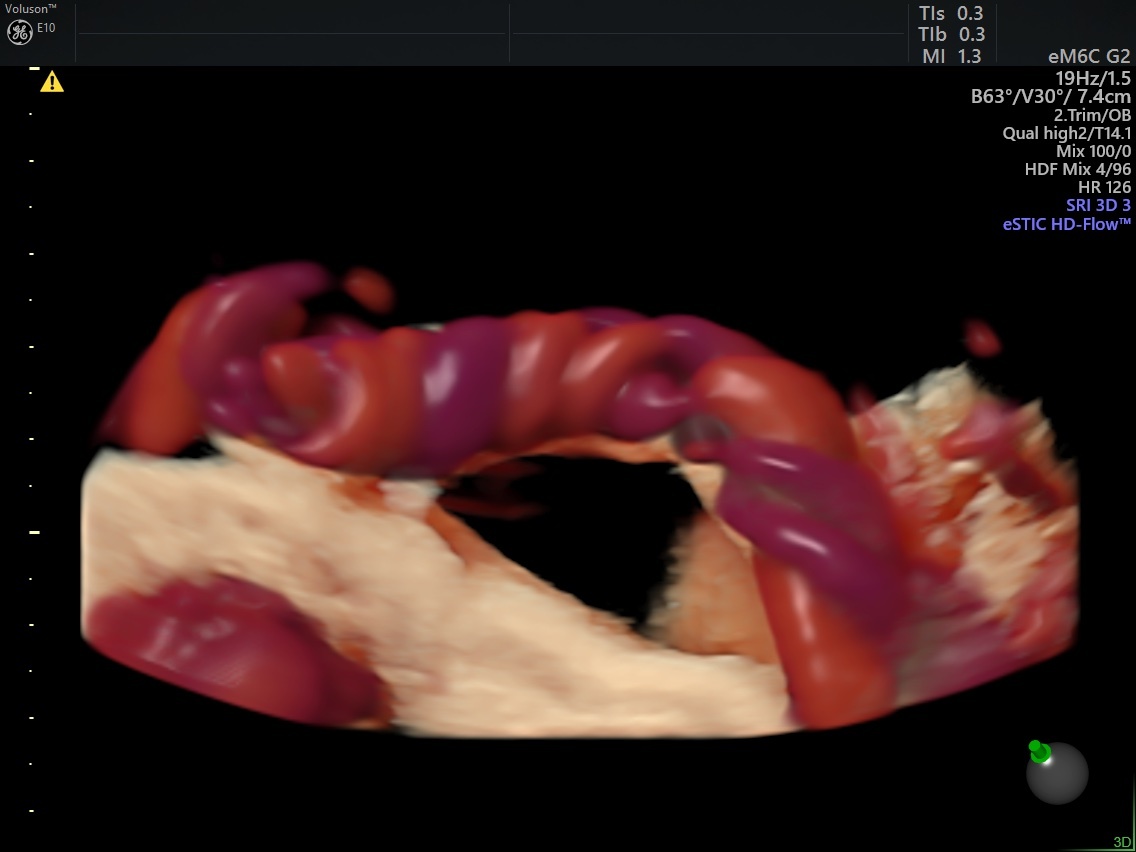
Umbilical Artery with Voluson™ HDlive™ Flow Silhouette technology.
The Importance of Doppler Assessment
The analysis of an umbilical artery Doppler assessment can provide a range of information on fetal circulation, including the presence, volume and direction of flow; velocity profile; and the impedance or resistance present.
As reflected by Doppler ultrasound findings, umbilical artery hemodynamics can effectively guide fetal and maternal care. Some of the benefits indicated include:
- Normal resistance to flow in the early second trimester of pregnancy is relatively high.
- Normal resistance to flow in the third trimester of pregnancy decreases.
- Highly resistive waveforms are always abnormal.
- When serial ultrasound exams demonstrate persistently reduced diastolic flow, that indicates real or potential fetal compromise and poor pregnancy outcomes.
- Any sign of diastolic flow reversal is representative of a severely compromised fetus.
In obstetrics, the use of umbilical artery Doppler — along with other fetal monitoring systems and appropriate and timely intervention — can predict and decrease perinatal mortality in certain high-risk pregnancies.