

All gynecologists know a patient who has suffered from debilitating cyclic dysmenorrhea, a classic symptom of endometriosis. The primary care physician has tried nonsteroidal anti-inflammatory drugs and continuous oral contraceptives, but the patient is still missing school or work monthly, and her quality of life is poor. She is then referred to you, as the gynecologist, for a workup.
So, what do you do to make the diagnosis? A 3D ultrasound of the pelvic anatomy, coupled with a careful pelvic exam, can help you streamline the process of diagnosing endometriosis and deliver the highest possible quality of care to your patient.
Evaluating Signs of Endometriosis
Endometriosis is an estrogen-dependent inflammatory process that is histologically defined by the presence of endometrial glands and stroma outside the endometrial cavity. Common sites for endometriosis to occur include the ovary and pelvic peritoneum. If adhesive disease or deep infiltrating endometriosis is present, it is most commonly found in the adnexa, bowel or pouch of Douglas.
Still, endometriosis does not always present in a typical fashion. Endometriosis can be found incidentally in asymptomatic patients. It may even occur in premenarchal or postmenopausal women, and it may occur outside of the pelvis. No single theory adequately explains the pathogenesis of endometriosis.
Surgery is neither the first nor second step in the process of evaluating severe dysmenorrhea complaints. A careful pelvic exam should be performed first. Signs of endometriosis include colored lesions in the posterior fornix, a cervix that is tethered to one side, pain on bimanual exam, nodules in the rectovaginal space, an adnexal mass or a soft, boggy uterus.
Streamlining Evaluation: 3D Ultrasound for Endometriosis
Seeing as there is no specific endometriosis diagnostic test, the next step is to use transvaginal ultrasound, including 3D ultrasound. Ultrasound allows the gynecologist to map out the areas of involvement and thus predict the extent of disease. A careful transvaginal ultrasound will determine areas of increased pain and nonmobile, tethered internal pelvic organs. This will assist the gynecologist in counseling the patient and planning treatment, whether medical, nonpharmacologic or surgical.
In addition, malformations of the female genital track, a common finding associated with pelvic endometriosis, can easily be diagnosed with 3D ultrasound. Ovarian reserve and ground glass adnexal masses consistent with endometriomas can be characterized with ultrasound. It can even detect the presence of adenomyosis or adhesive disease, such as the frozen pelvis, and evaluate the bladder mucosa long before a scalpel ever touches the patient's skin.
Lastly, tubal patency can be determined by performing hysterosalpingo-contrast-sonography if there is concern about fertility. All this information can be gathered in your office relatively quickly, allowing you to streamline the evaluation process and counsel the patient regarding your diagnosis and recommendations.
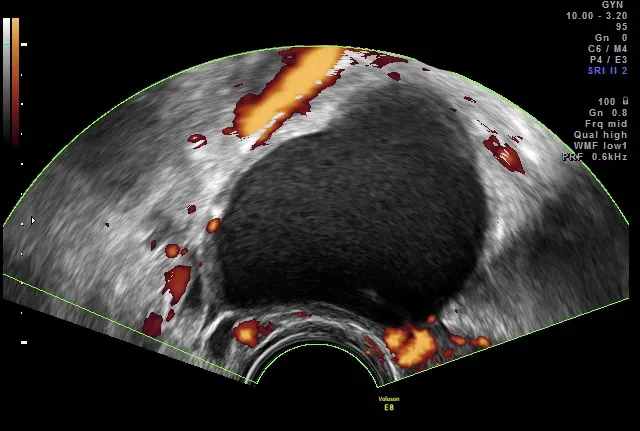
3D ultrasound image of endometrioma
Image courtesy Dr. Stefano Guerriero
Diagnosing Endometriosis
A presumptive diagnosis of endometriosis is made using a combination of the patient's symptoms, a physical exam and ultrasound findings. The presence of typical adnexal masses consistent with endometriomas helps confirm the diagnosis. Atypical endometriomas that are multiloculated and contain cystic and solid areas or ultrasound findings of endometriomas in postmenopausal women always raise the suspicion of malignancy. These situations require more immediate surgical intervention.
Otherwise, histologic diagnosis is not required, especially if infertility is not the primary issue and the treatment plan is to use low-risk medical therapy. If symptoms do not improve with medical therapy, surgery is the next course of action. Depending on your surgical skill level and the patient's desire, you can schedule the patient for the operating room or consult with an expert in surgical management of extensive endometriosis.
Gynecologists need to be accurate, prompt and confident when caring for patients suffering from cyclic dysmenorrhea. Clinical acumen, combined with a careful pelvic ultrasound that includes 3D imaging, can make the diagnosis of pelvic endometriosis a cinch.



