

Even on a good day, trying to diagnose stomach pain in women can be difficult. There are so many potential causes and overlapping issues, and training in diagnosing stomach pain and management of this symptom has been inconsistent at best. When patients complain of stomach pain, physicians should always consider the possibility of both intestinal endometriosis and Crohn's disease, which is an inflammatory bowel condition. Like diabesity (the genuine coexistence of diabetes and obesity), chronic abdominal pain may be due to the presence of both Crohn's disease and endometriosis, specifically intestinal endometriosis, a disorder of retrograde menstruation involving the bowel.
Normal Bowel Wall

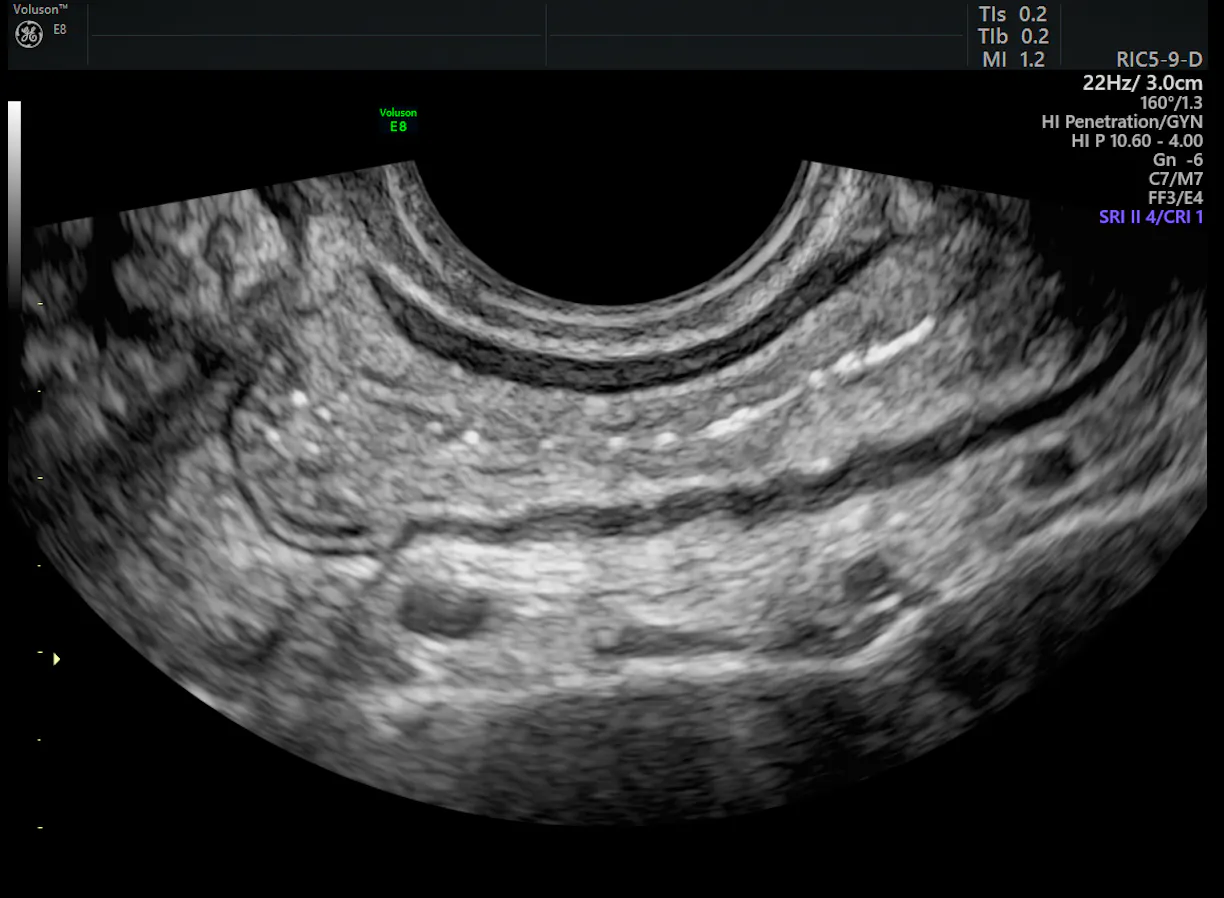
Deep Infiltrating Endometriosis Ultrasound
The Prevalence of Endometriosis and Crohn's Disease
According to a 2011 article published in the World Journal of Gastrointestinal Surgery, the exact incidence of intestinal endometriosis is unknown. The authors estimated that up to 37 percent of women with endometriosis have intestinal endometriosis, with the most common locations in order of prevalence being the sigmoid colon and the rectum, then the ileum, the appendix and the cecum.
In 2000, an article in the European Journal of Gastroenterology & Hepatology described the presence of intestinal endometriosis in the terminal ileum of eight patients taken to surgery for complications connected to Crohn's disease. The diagnosis of intestinal endometriosis had not been made prior to the surgery. Subsequent pathology of the resected bowel, however, confirmed the presence of both disorders.
More recent research also suggests a strong association between endometriosis and other intestinal disorders. Medscape summarized the results of a nationwide longitudinal study in Denmark, published in 2011. The researchers found that women with endometriosis may be 80 percent more likely to develop inflammatory bowel disease compared with women without endometriosis.
Different Conditions, Similar Symptoms
Crohn's is an intestinal disease often affecting all layers of the terminal ileum and colon. As noted in the article from the World Journal of Gastrointestinal Surgery, intestinal endometriosis is defined as the presence of endometrial-like glands and stroma involving the subserosal fat and deeper tissue of the intestinal wall. Hence, endometriotic implants concerning the serosa alone are classified as peritoneal endometriosis. Not surprisingly, intestinal endometriosis is often found alongside endometriosis involving the pelvic peritoneum and ovaries.
Presenting symptoms of intestinal endometriosis vary and can mimic those of Crohn's disease: crampy abdominal pain, dyschezia, painful bowel movements, constipation, diarrhea, bloating, passage of bloody stools and rectal bleeding. Crohn's disease often waxes and wanes, with many women finding an association between worsening symptoms and their menstrual cycles.
Using Ultrasound for Diagnosis and Treatment
A multidisciplinary team — including members of physiotherapy, nursing, radiology, gynecology, gastroenterology, urology and colorectal surgery — is essential when addressing these complex diseases. A high index of suspicion followed by a careful history and an exam are key components for making a judgment. These steps alone, however, are inadequate for making a diagnosis of intestinal endometriosis.
Radiologic imaging is a necessary part of the evaluation, and 3D ultrasound is one of the most commonly used and relied upon techniques. Ultrasonic gel and water contrast instilled in the vagina or rectum may be especially helpful in diagnosing intestinal endometriosis, particularly when assessing for bowel lesions or deep infiltrating endometriosis. Furthermore, patients often find that transvaginal ultrasound is a more comfortable exam than an MRI. Typically, colonoscopy will not identify intestinal endometriosis unless a large transmural nodule is present, but it can reveal mucosal inflammation and — when coupled with biopsy — diagnose the presence of Crohn's disease.
Multiple hormonal therapies may help alleviate symptoms, but they do not appear to stop the progression of intestinal endometriosis and cannot be used long term in women seeking to conceive. Surgical evaluation with nodulectomy or segmental bowel resection are treatment options if intestinal stenosis exists. A laparoscopic approach typically results in a shorter recovery while providing equally excellent results compared to laparotomy.
Why do these two conditions occur together? That question has not yet been answered. So far, the medical field knows that both are chronic in nature, involve inflammatory processes and present in the young adult. If treatment fails for endometriosis and abdominal pain is still present in your patient, remember to consider that possibility. The underlying issue may be both intestinal endometriosis and Crohn's disease.



