
IVF protocols vary depending on a patient's age, diagnosis and a variety of other factors. Most often, however, protocol calls for ovarian stimulation rather than natural cycle IVF.
During traditional IVF, a patient injects exogenous hormones — including follicle-stimulating hormone (FSH), luteinizing hormone (LH) or a combination of both — for around nine to 12 days to stimulate the ovaries. Throughout this cycle of injections, the ovaries and uterine lining are monitored via transvaginal ultrasound and blood work.
Once a patient has enough mature follicles, they will inject human chorionic gonadotropin (hCG) and possibly another medication such as Lupron to mature the smaller follicles. The oocyte retrieval and eventually the transfer are performed under ultrasound guidance.
However, the option exists to exclude exogenous hormones and follow the patient's natural cycle. Natural cycle IVF differs from traditional IVF in a few key ways and may be a better choice for some patients.
What Is Natural Cycle IVF?
This IVF approach forgoes the use of exogenous hormones, relying instead on a woman's natural cycle. Otherwise, this alternative protocol is relatively similar to traditional IVF. During a natural cycle protocol, the reproductive endocrinologist monitors the patient's follicular development via ultrasound and blood work. Typically, only one follicle is produced, although some patients may produce two.
When at least one follicle is mature, the patient undergoes an egg retrieval under ultrasound guidance. The egg is fertilized in the lab and transferred back into the patient if the embryo develops properly into a blastocyst. If there are two embryos, the other is frozen for later use.
Modified natural cycle IVF, an alternative form of this approach, includes hCG or gonadotropin-releasing hormone (GnRH) antagonists just as traditional IVF does.
The first baby born following natural cycle IVF was Louise Brown, also known as the world's first "test-tube baby." Over time, reproductive endocrinologists drifted away from this protocol and began using ovarian stimulation medications to produce more eggs. The hope was to produce more eggs per cycle and increase the chance of a live birth. However, in recent years, more physicians have returned to a natural cycle protocol to reduce the potential health risks to patients.
Benefits and Drawbacks of Natural Cycle vs. Traditional IVF
According to preliminary 2017 cycle data from the Society for Assisted Reproductive Technology, frozen embryo transfers following natural cycle IVF resulted in a higher live birth rate than fresh transfers, regardless of the patient's age.
Like natural cycle IVF, traditional IVF frozen transfers are more successful than fresh. Interestingly, the live birth rates of frozen cycles for traditional IVF are similar to those of frozen cycles following a natural cycle protocol.
There are pros and cons to both protocols. Natural cycle IVF involves no stimulation medications, which reduces patients' costs, number of office visits and side effects. These cycles also have a reduced risk of multiple births and low birthweight babies. Patients who undergo natural cycle also tend to experience lower levels of depression and higher levels of patient satisfaction during treatment, according to one study.
The live birth rates of natural cycle in vitro fertilization are similar to traditional IVF following frozen transfers. However, women undergo an average of 3.5 cycles of natural cycle IVF before they have a live birth, compared to the average 2.9 cycles they might undergo of traditional IVF, according to a study published in Human Reproduction. These cycles also have an increased risk of premature ovulation and therefore a greater likelihood of being canceled compared to traditional IVF.
One caution is that the single egg often produced in a natural cycle might not be healthy enough to become a top-quality blastocyst, nor will there likely be any embryos to freeze. If these patients opt for a fresh transfer, the chances of a live birth are lower than with traditional IVF. Additionally, preimplantation genetic testing is typically not recommended in a natural cycle, and the embryo transferred might not be euploid.
Traditional IVF offers a reduced chance of cycle cancellation compared to natural cycle, and embryos not transferred can be frozen for later use. There are higher live birth rates associated with fresh transfers during traditional IVF when compared to natural cycle. Traditional IVF patients also have the option of diagnosing chromosomal and genetic abnormalities through preimplantation genetic testing.
Because traditional IVF cycles use stimulation medications, however, patients experience increased costs, office visits and possible side effects, including ovarian hyperstimulation syndrome (OHSS). When transferring more than one embryo, patients also are at an increased risk of having multiple pregnancies.
When to Recommend Natural Cycle IVF
Reproductive endocrinologists should consider recommending a natural cycle protocol when patients are younger than 35 and can ovulate on their own. Natural cycle IVF may also be appropriate for patients who are at risk for an exaggerated response to ovarian stimulation medication, such as those with polycystic ovarian syndrome (PCOS).
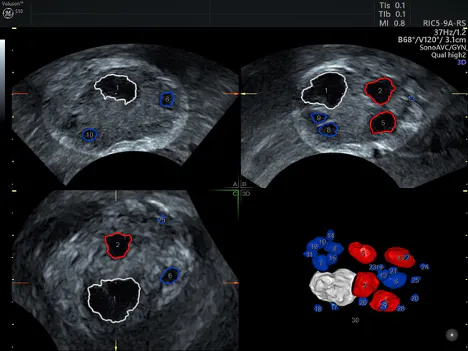
3D view of ovary using SonoAVC™ antral (Sonography-based Automated Volume Calculation) demonstrating the dominant follicle in white
Natural cycle can be considered for patients who do not wish to take ovarian stimulation drugs. Patients may also be interested in this form of IVF if they want to produce only one embryo for ethical or religious reasons.
Physicians should consider recommending traditional IVF when patients are of advanced reproductive age and have damaged or blocked fallopian tubes, or unexplained infertility. Traditional IVF is also a better path forward for patients who have been diagnosed with an ovulatory disorder, have hormonal imbalances, have an inheritable genetic disorder or want to produce more than one embryo to freeze for later use.
It's important to note, however, that research published in Best Practice and Research: Clinical Endocrinology and Metabolism strongly encourages physicians to consider the patient's prognosis over their personal preferences. The American Society for Reproductive Medicine asserts that a physician may ethically refuse to proceed with any type of IVF cycle if the patient's chance of success is extremely low.
Be candid with your patients about their IVF prognosis, and provide them with as much information as possible to help them make an informed decision about their treatment. Remind them that natural cycle IVF is just one option in the array of assisted reproduction technology treatments available.

