
By the time a patient reaches menopause, their likelihood of being diagnosed with endometriosis wanes considerably. In fact, according to a review from Diagnostics, just 2 to 5 percent of postmenopausal patients are affected by endometriosis. This is compared to the 10 to 15 percent of reproductive-age patients who have endometriosis, according to a review in Current Obstetrics and Gynecology Reports. These gaps represent the estrogen-dependent nature of the disease and its reduced prevalence amid declining hormonal levels after menopause.
Despite the rareness of this diagnosis, however, endometriosis after menopause has been clinically recognized for decades: The first documented case reported in 1942, the Diagnostics review notes. Even so, there remains a limited amount of literature available on the condition, which raises ongoing questions related to diagnosis and treatment.
These questions are further complicated by the risks inherent in postmenopausal endometriosis, including malignant transformation and impacts on patients' quality of life.
Recognizing Postmenopausal Endometriosis
Postmenopausal patients with endometriosis often present similarly to patients of reproductive age. Signs and symptoms include pelvic discomfort and ovarian cysts, as well as digestive complaints, such as nausea, diarrhea or constipation. In some cases, postmenopausal endometriosis may appear as menopausal symptoms, such as hot flashes. Some patients may have no symptoms at all.
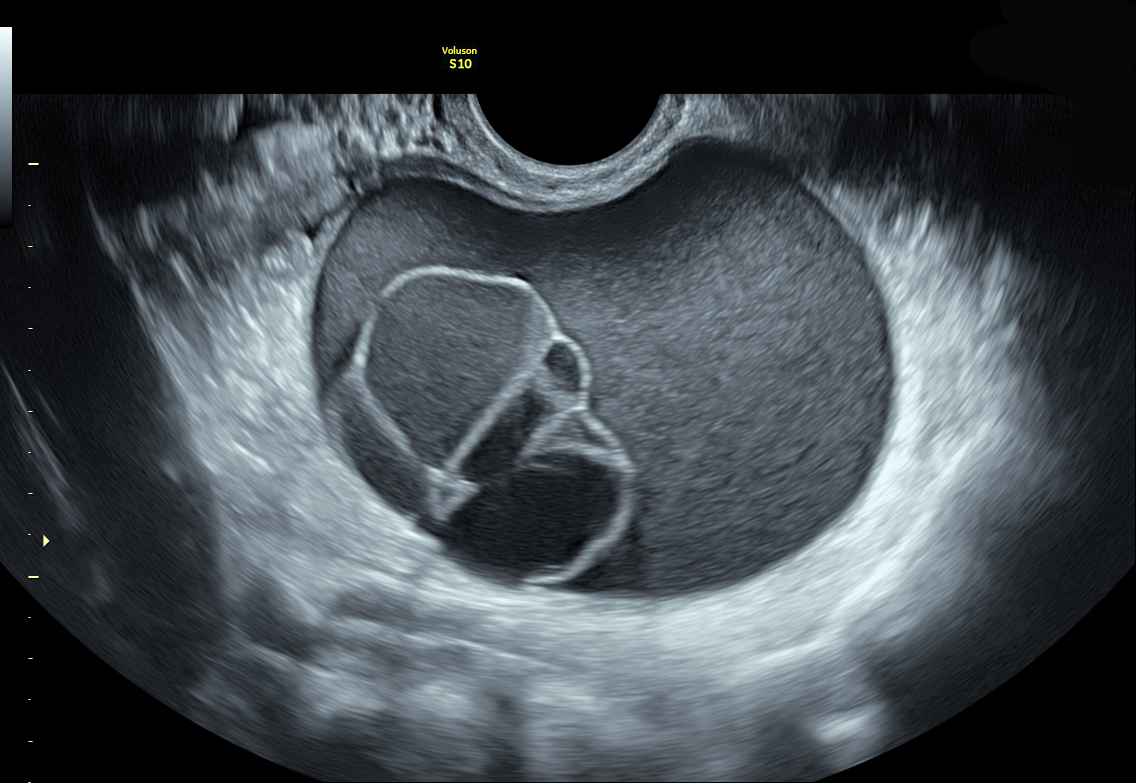
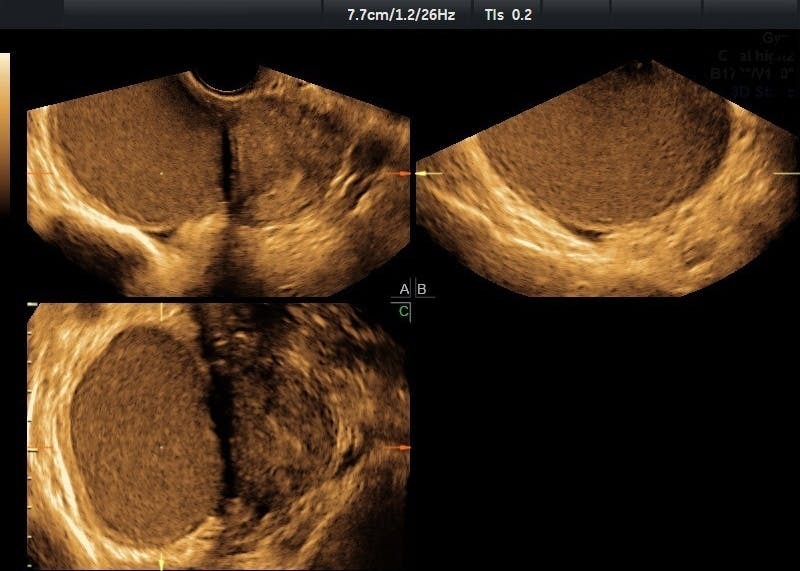
Ovarian Cyst shown on ultrasound - could present similar signs and symptoms to postmenopausal endometriosis
Endometriosis after menopause can occur in patients who were diagnosed in their premenopausal years, as well as those who were not. However, it is unknown whether new diagnoses stem from undiagnosed endometriosis from a patient's reproductive years or an actual de novo disease state. Risk factors can include those that affect estrogen levels, such as hormone therapy or obesity. Another theory detailed in a study published in Gynecological Surgery holds that endometriosis several years post-menopause may be due to unknown genetic and epigenetic incidents affecting estrogen sensitivity or production.
Among the potential risks of endometriosis is the chance that the lesions could become cancerous and metastasize. Clinicians should consider the slight but elevated risk of malignancies in endometriosis patients, as well as the fact that estrogen therapy may increase that risk. According to a report from Hormone Molecular Biology and Clinical Investigation, the risk of endometriosis transforming into ovarian cancer is quantified at 2 to 3 percent.
Diagnosing Postmenopausal Endometriosis
Risks of malignancy and quality-of-life impacts may be exacerbated by the fact that endometriosis is not often detected in the early stages. Those delays become more prevalent as patients age.
Laparoscopy can aid in the timely diagnosis of endometriosis, including for postmenopausal patients. Transvaginal ultrasound may also support noninvasive diagnostic decision-making, although clinicians should recognize the variances in lesion abnormalities among older patients compared to younger patients. One such distinction is the appearance of a "ground glass" ovarian cyst. After menopause, those characteristics are linked to a 44 percent risk of malignancy, according to the study published in Diagnostics.
Typical
The majority (nearly 8 in 10) of postmenopausal endometriosis patients develop ovarian endometriomas, although lesions may also appear elsewhere. Rarely, the condition may spread to tissues outside of the pelvic region, such as the colon or bladder. These uncommon cases are sometimes seen in postmenopausal patients, as it can take years for endometriosis to spread to these areas.
Treating Endometriosis After Menopause
Management strategies for postmenopausal patients with new or recurrent endometriosis diagnoses vary. For symptomatic patients without a clinical history of endometriosis, surgery may be an option to alleviate symptoms and reduce the risk of malignant transformation. Non-surgical options such as progesterone or aromatase inhibitors have also been discussed as options, though some therapies may come with bone density concerns or other risks.
For patients with a history of endometriosis, the use of hormonal replacement therapy during menopause is widely debated. Given the estrogen-based mechanics of hormonal therapy, some researchers point to questions about its effect on symptom and disease recurrence, as well as cancer risk. However, the use of hormone replacement therapy carries many benefits for postmenopausal patients, including supporting bone health.
Some researchers suggest patients should not be denied therapy just because they have previously had endometriosis. In a review from Medicina, the authors weighed those benefits and risks documented in low-grade literature to arrive at a recommendation of using combined estrogen and progestogens rather than unopposed estrogen. Still, more research is needed in this area.
Bottom Line: Does Endometriosis Go Away After Menopause?
Instances of endometriosis very often diminish as estrogen reduces during menopause, but a small percentage of postmenopausal patients will still experience the condition, either as a new diagnosis or one that recurs. The reasons are not entirely understood just yet, but it may be due to endogenous or exogenous estrogen sources as well as genetic behaviors that influence how estrogen is used and produced in the body.
Importantly, clinicians should acknowledge that although rare, postmenopausal endometriosis can contribute to a negative quality of life through pelvic discomfort, gastrointestinal complaints and other unwelcome symptoms. Additionally, there is a risk of malignancies from endometrial lesions.
Diligent surveillance for rare conditions is a critical part of holistic patient care, especially for clinicians such as gynecologists who treat patients over many years and stages of life. With reliable and accessible diagnostic tools, such as ultrasound, providers can make more informed decisions to guide comprehensive care planning related to endometriosis and other diagnoses dependent on early detection.

