
Chronic menstrual pain and severe dysmenorrhea are the leading symptoms of adenomyosis. Yet, because pain and bleeding are not unusual, these symptoms have become normalized and sometimes even trivialized, meaning some women can suffer for years before receiving adenomyosis treatment. Fortunately, ultrasound technology is opening up new paths to adenomyosis diagnosis and treatment.
The Challenges of Identifying Adenomyosis
Adenomyosis occurs when ectopic endometrial glands and stroma develop in the myometrial layer of the uterine wall, where they are commonly surrounded by hyperplastic tissue. It is a disease of the inner myometrium, in which the basal endometrium infiltrates into the underlying muscle and is followed by hypertrophy and hyperplasia. Endometrial glands that are more than 2.5 mm below the endometrial-myometrial junction are a key diagnostic criterion for adenomyosis, according to a paper published in BioMed Research International.
However, adenomyosis is not a uniform pathology, but represents a spectrum of disease. Cases can range from focal adenomyomas to diffuse overall adenomyosis, which can include disruption of the junctional zone with either a small or large amount of endometrial invasion.
In particular, the disruption and thickening of the junctional zone have come to be strongly associated with adenomyosis. Evaluation of the junctional zone is a key part of adenomyosis diagnosis and treatment.
Ultrasound's Role in Adenomyosis Diagnosis
Adenomyosis is a relatively frequent finding in hysterectomies performed for menorrhagia and dysmenorrhea. Traditionally, adenomyosis is diagnosed after hysterectomy. Some studies have shown that a diagnosis can be made with biopsies done at hysteroscopy and laparoscopy. Non-invasive imaging can also be used to help guide a differential diagnosis.
Clinical diagnosis and adenomyosis treatment are usually difficult due to the nonspecific nature of symptoms and the confounding factor of coexisting pelvic diseases. Roughly one-third of cases are asymptomatic, with the remaining two-thirds linked to dysmenorrhea, menorrhagia, chronic pelvic pain and uterine enlargement.
Coexisting pelvic diseases, including endometriosis and uterine fibroids, occur in about four out of five cases of adenomyosis, according to a study published in Advances in Clinical and Experimental Medicine. The incidence of adenomyosis is not as clear; estimates of its prevalence vary widely.
Women between the ages of 35 and 50 compose the majority of cases, especially multiparous, premenopausal women. Multiparity is thought to be a causal factor due to the trophoblast invasion into the myometrium. Hormones have also been shown to be a cause, as adenomyosis tissue has been found to contain estrogen receptors. There also appears to be a connection between the condition and previous uterine surgery such as cesarean section.
Historical Treatment Methods for Managing Adenomyosis
Originally, adenomyosis was only treated by hysterectomy. This initial surgical treatment expanded into wedge resection, which allowed for partial removal of adenomyosis nodules. More recently, treatment advancements have come to include uterine-sparing and minimally invasive options such as laparoscopic surgery.
Nonsurgical treatment methods focus on controlling the menorrhagia with contraceptive pills, hormonal patches, oral progesterone or levonorgestrel intrauterine devices (IUD) along with non-steroidal anti-inflammatory drugs (NSAIDs) for pain relief.
When conservative treatment is not effective or preferred, surgery can be considered. Endometrial ablation or resection, concurrent myometrial excision or uterine artery ligation can all be used with varying success rates. Superficial adenomyosis can be treated by endoscopic endometrial ablation. For a patient presenting with both adenomyosis and uterine myoma, uterine artery embolization (UAE) is a common treatment method.
Adenomyomectomy is another conservative surgical management that can be considered. Traditionally done as an open adenomyomectomy and first recorded in 1952, it was once considered the gold standard for treating extensive disease. However, some adenomyomectomy techniques come with a risk of uterine rupture and result in more external scarring and internal adhesions than other treatment methods.
The modification to laparoscopic adenomyomectomy with endoscopy has been found to be a good option for treating adenomyomas, especially for patients who may want to become pregnant in the future. The procedure appears to be both feasible and safe in the debulking of an enlarged uterus and correcting physical impediments to sperm transport, with a limited rate of recurrence and good follow-up results.
However, uterine surgery can increase the risk of uterine rupture during future pregnancies. The removal of any significant portion of the myometrium will reduce myometrial ability, as well as result in a uterine scar that can reduce the tensile strength of the lower uterine segment. If a patient wants to retain fertility, it is crucial to prevent tubal damage, ensure the myometrial wall is properly reconstructed, maintain the uterine cavity and minimize postoperative adhesions.
Because of the range of available treatment options for adenomyosis, hysterectomy is now usually considered a last resort. It may be a viable option if other treatments have been unsuccessful in controlling symptoms, or if the patient is not a good candidate for any other medical or surgical management.
Imaging Modalities for Diagnosing and Managing Adenomyosis
Adenomyosis was historically diagnosed using post-hysterectomy histology, then MRI. Now, a pre-surgical diagnosis can be made with transvaginal ultrasound. A study published in Ultrasound in Obstetrics and Gynecology reports that the specificity and sensitivity of transvaginal ultrasound are comparable to those of MRI and histology; 3D transvaginal ultrasound has an overall accuracy of 89 percent for diagnosing adenomyosis. Besides these advantages, ultrasound is often widely available and convenient for providers as a first-stage method of uterine assessment.
According to a study published in Facts, Views and Vision, the major tell-tale sonographic features of adenomyosis include:
- A heterogeneous myometrium.
- Myometrial cysts.
- Globular uterine enlargement, greater than 12 cm in length.
- An asymmetrical anteroposterior myometrium, with the anterior wall appearing thinner than the posterior wall.
- An endometrial junction that is difficult to identify.
- A thickened transitional zone. (When the hypoechoic layer surrounding the endometrium measures greater than 12 mm, it is strongly associated with adenomyosis.)
- Subendometrial echogenic linear striations.
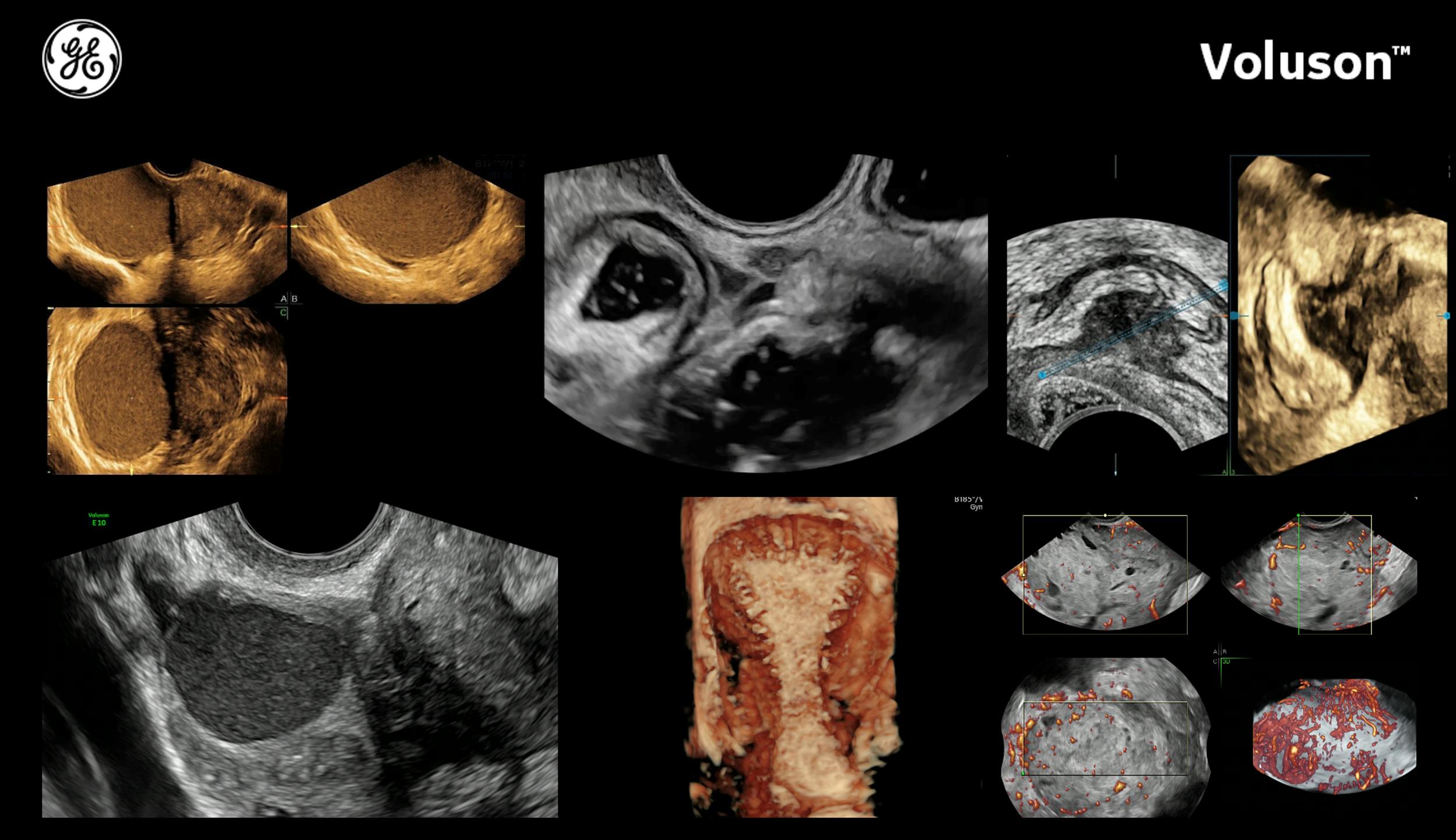
MRI uses the features and measurements of the junctional zone to determine the extent of adenomyosis, while 2D ultrasound focuses on the heterogeneity of the myometrium. 3D ultrasound provides significantly more information about the junctional zone.
The Ultrasound in Obstetrics and Gynecology study notes that myometrial cysts are the most specific 2D ultrasound feature when diagnosing adenomyosis, while the most sensitive feature is a heterogeneous myometrium. The major advantage provided by 3D ultrasound, besides the added view of the coronal plane, is its ability to reveal the degree of junctional zone infiltration and distortion.
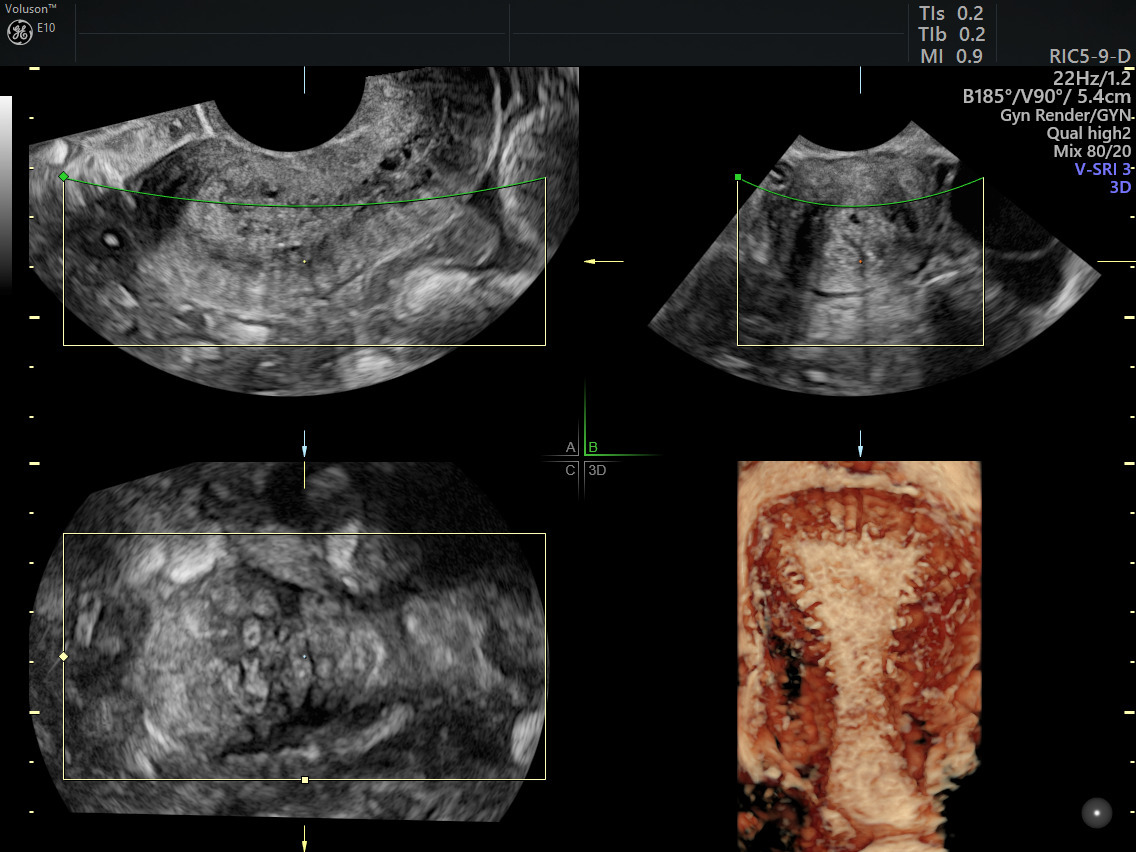
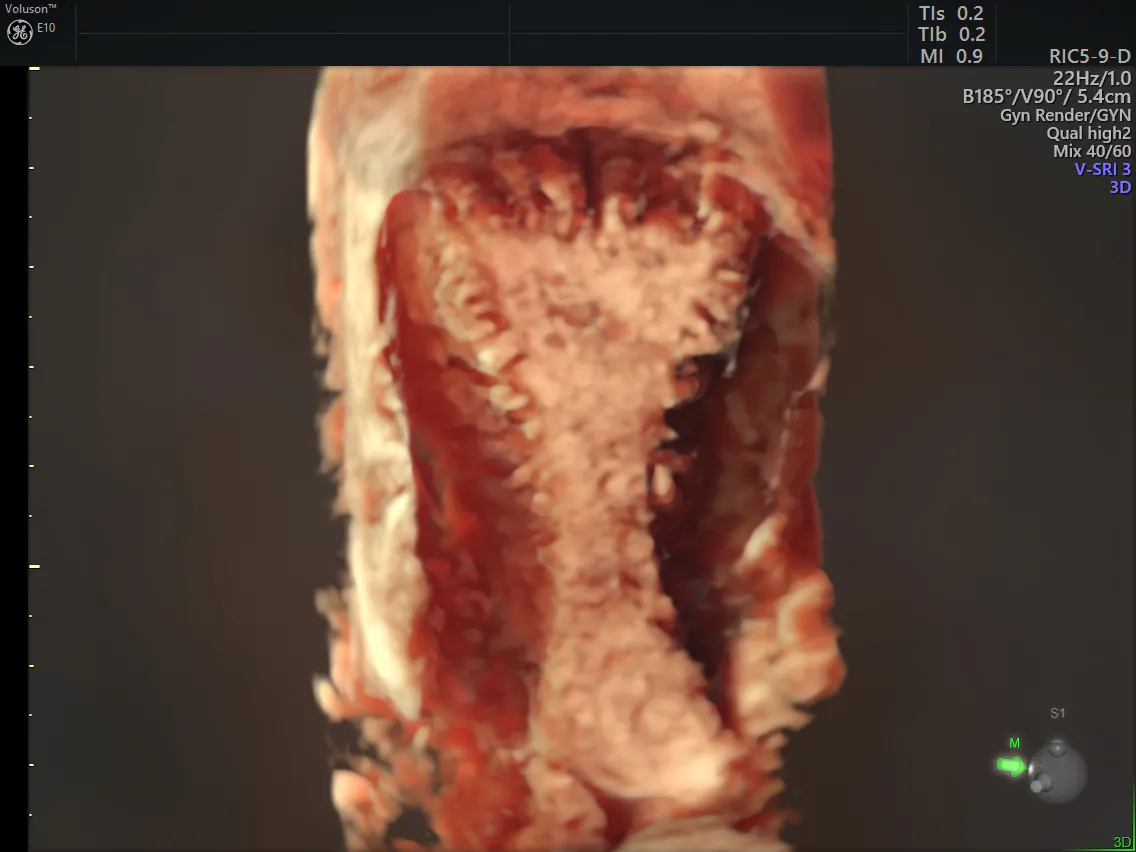
Adenomyosis shown on ultrasound using 3D HDlive™
The addition of color Doppler reveals the vascularity of any masses, which helps clinicians better differentiate adenomyomas from uterine myomas. In a focal adenomyoma, the vessels are diffusely arranged within the mass and follow their normal course perpendicular to the endometrium. A color Doppler scan of a myoma will show vessels that circumscribe the mass.
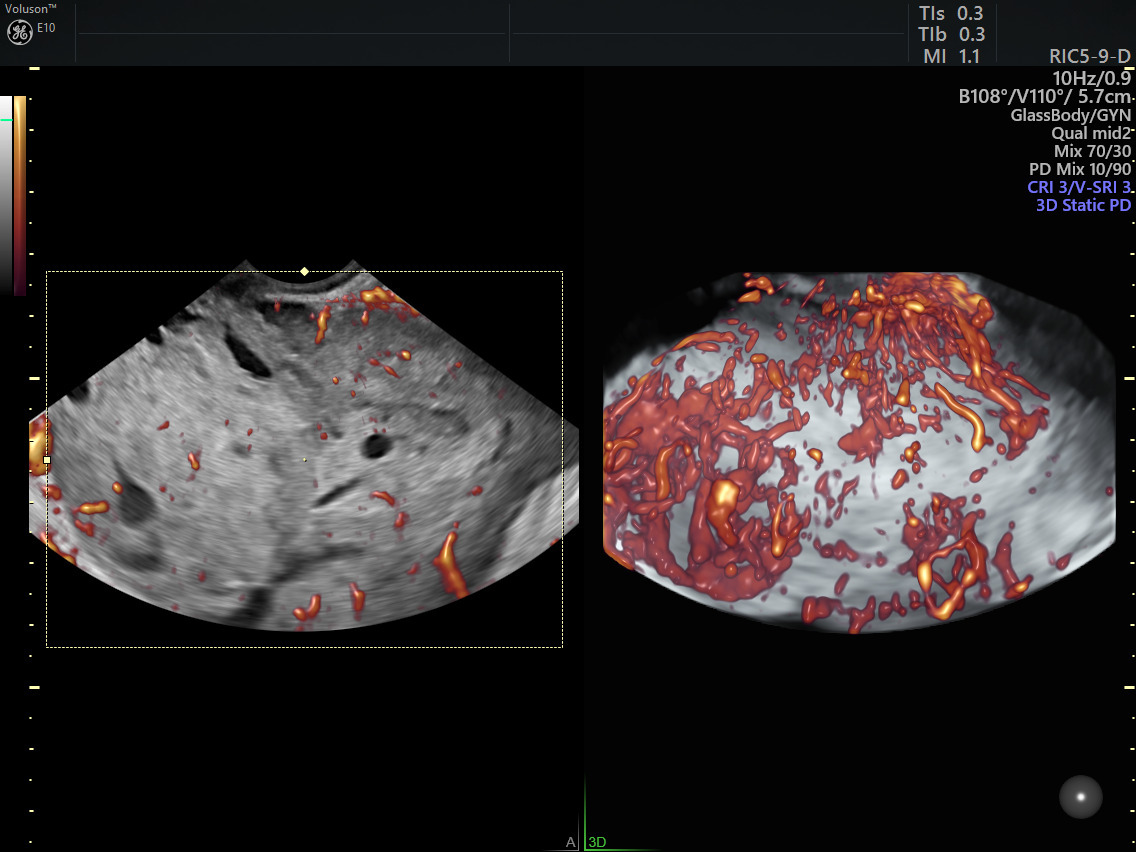
Adenomyosis shown on ultrasound using color Doppler
Uterine myomas appear on ultrasound as hypoechoic or isoechoic masses with posterior shadowing and can have calcifications or be calcified. In comparison, adenomyomas have streaky posterior shadows and no calcifications.
A Path to Long-Term Success in Adenomyosis Treatment
Diagnosing and treating adenomyosis is still a challenge across the gynecology field. Clinicians should be on the watch for ultrasound characteristics suggesting its presence to allow for early diagnosis.
Careful understanding of ultrasound markers is necessary to differentiate between focal adenomyomas and uterine myomas, which frequently occur together and can require different treatments.
Adenomyosis treatment has improved significantly since this disease was first identified, allowing women more choices and more control over their bodies, fertility and futures.