

Endometriosis is a chronic inflammatory disease in which ectopic endometrial cells outside of the uterus respond to hormonal stimulation with various degrees of cyclic hemorrhage, often forming an endometrioma. The "typical" endometrioma is an ovarian cyst containing low-level echoes.
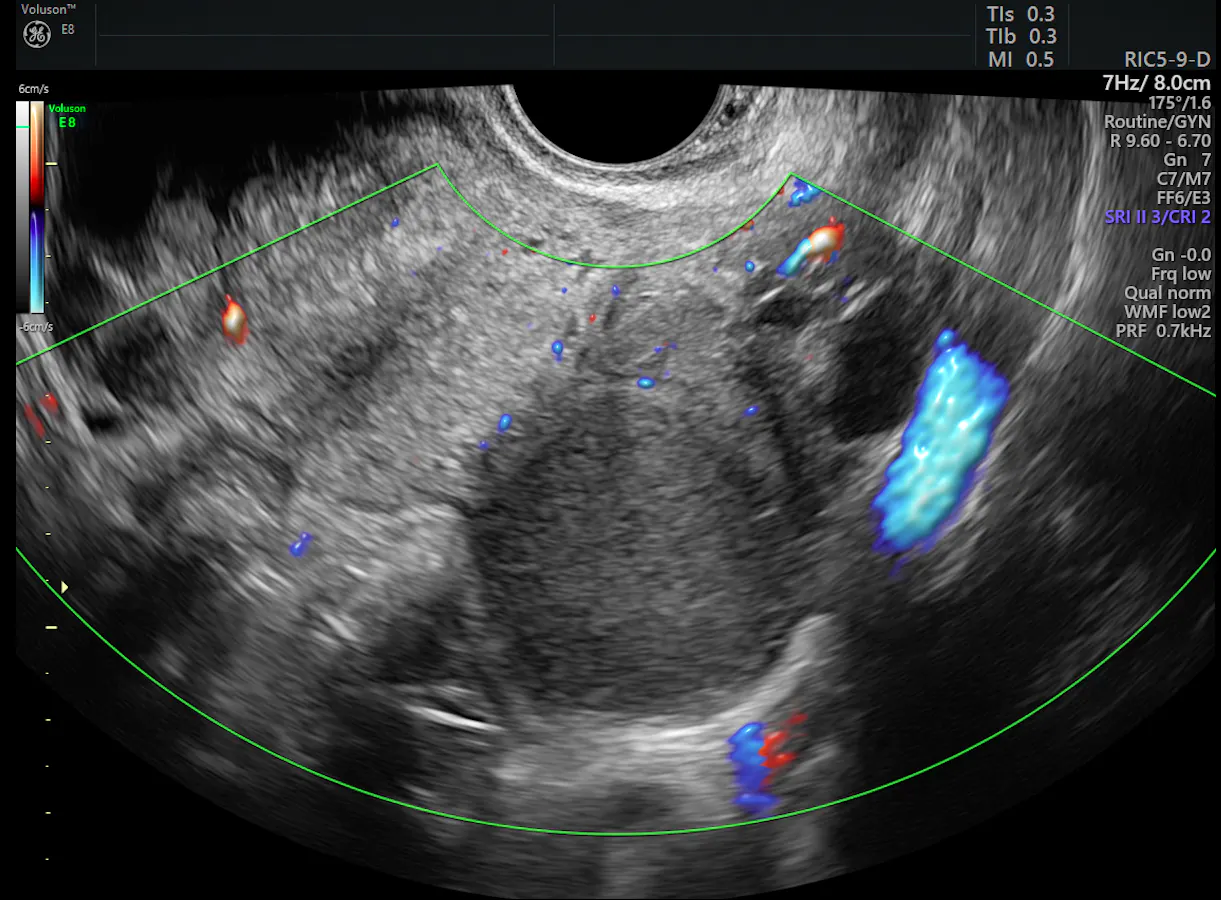
Endometrioma within ovary on ultrasound
Assessing an endometrioma requires careful transvaginal ultrasound imaging as the patient will typically have significant pain and hemorrhage. And that is the easy part of endometriosis imaging. The challenging part is determining the extent of non-ovarian disease and how far it has spread into pelvic structures.

Small endometrial implant in posterior vaginal fornix
What Types of Pain Does Endometriosis Cause?
Deep infiltrating endometriosis occurs when endometrial cells implant into the fibromuscular pelvic structures, such as rectovaginal septum, uterosacral ligaments, vagina, urinary tract, bowel and rectum. The location of these endometrial implants will affect the types of symptoms that a patient experiences. For example, if the lesions occur on the pelvic wall, the patient will feel somatic pain, often described as a sharp pain. If the lesions form on organs (uterus, bowel, bladder), visceral pain will occur, a dull or cramping pain that can lead to nausea and vomiting.

Image of normal bowel wall
Deep Infiltrating Endometriosis in bowel wall
Other nonspecific symptoms can also be caused by ectopic endometrial implants, such as bowel and bladder dysfunction, pain with urination, pain during intercourse, gastrointestinal distress, chronic fatigue and infertility. This variation in symptoms is one of the reasons why endometriosis can be so difficult to diagnose. It also explains why many patients often do not know that endometriosis could be responsible for their symptoms.
Keeping Communication a Priority
Although endometriosis is not completely understood, the cause is probably multifactorial, and multiple theories have been proposed. Of these, the oldest and most widely accepted is the retrograde menstruation theory, according to Fertility and Sterility. This theory suggests that endometriosis occurs when retrograde menstruation releases endometrial cells out through the fallopian tubes into the pelvis, which can then implant onto organs or the peritoneal surface. Evidence for this theory is demonstrated by the greater number of women with endometriosis who have excessive retrograde flow due to obstructive mullerian duct disorders, and the pattern of endometrial implant distribution within the dependent areas of the pelvis.
Explaining endometriosis to patients is often best achieved with a clear visual of the pelvis and pelvic organs to demonstrate the relationship between the uterus and the surrounding area. It is also a good idea to provide some basic innervation information on the types of pain associated with different tissue damage. In this way, you can help your patient understand how the many variable symptoms can all be expressions of endometriosis's pathology. Additionally, having access to in-house imaging technology can support this explanation with a diagnostic assessment of the patient's areas of pain, ensuring that treatment can be arranged before the patient even leaves the office.
The Link Between Endometriosis and Pelvic Floor Dysfunction
Deep infiltrating endometriosis can lead to pelvic floor dysfunction due to the chronic inflammatory reaction that ectopic endometrium causes in surrounding tissues. This leads to the development of adhesions, inflexible scar tissue, high-density nodules and even the destruction of normal tissue or organs.
As reported in Deutsches Arzteblatt International, endometrial implants on the ureters or intestinal walls can cause stenosis and painful and ineffective bladder and bowel wall contractions. Implants on the ligaments and peritoneal surfaces of the pelvis lead to rigid adhesions. If enough soft tissue is replaced with fibrotic nodules, the pelvic organs can become fixed to the pelvic bones, making them immobile or "frozen."
How Ultrasound Helps to Assess the Pelvic Floor
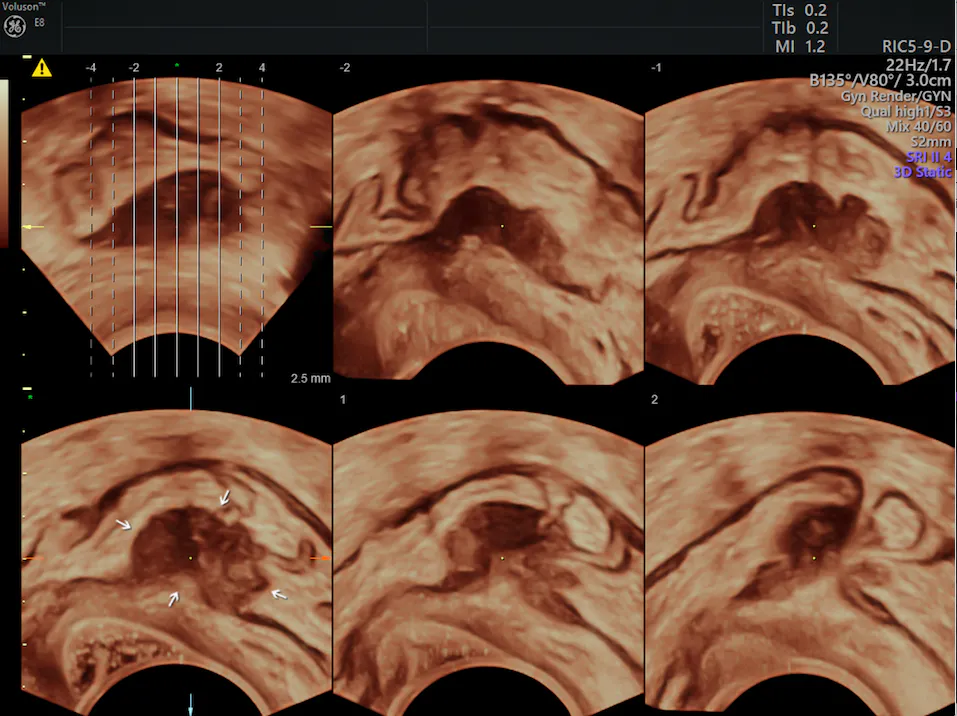
To be able to accurately assess pelvic floor dysfunction caused by deep infiltrating endometriosis, or simply pelvic endometriosis, a dynamic tool is necessary — one that allows for multicompartmental assessment. As reported by BJR, ultrasound is a modality well-suited for these requirements as it is safe, inexpensive and capable of performing a first-line evaluation.

Dynamic movement demonstrating lack of movement of endometrial implant
Ultrasound is flexible enough to assess the anatomy and function of the entire pelvic floor in real-time, which ensures that you can address all aspects of dysfunction to allow for optimal treatment and results. Transvaginal ultrasound provides bladder neck views anteriorly and bowel and rectum views posteriorly. The transperineal view shows the anterior, middle and posterior compartments of the pelvis, and the endoanal ultrasound can further assess the sphincter complex surrounding the anal canal.
Only by having a clear picture of all parts of the pelvic floor can the effects of a patient's deep infiltrating endometriosis be completely understood. Use ultrasound to make a thorough diagnosis and develop a well-balanced treatment plan.



