
The Tetralogy of Fallot prognosis has changed significantly since the rare condition was first discovered — still, this diagnosis remains challenging for both parent and baby.
Tetralogy of Fallot (TOF) is classified as a critical congenital heart defect (CCHD). According to the Centers for Disease Control and Prevention (CDC), congenital heart defects occur in about 1 percent of all births in the US, and a quarter of these are CCHDs. Congenital heart defects also account for around 4 percent of deaths during the neonatal period, and while some are mild, CCHDs — and TOF in particular — typically require surgery soon after birth.
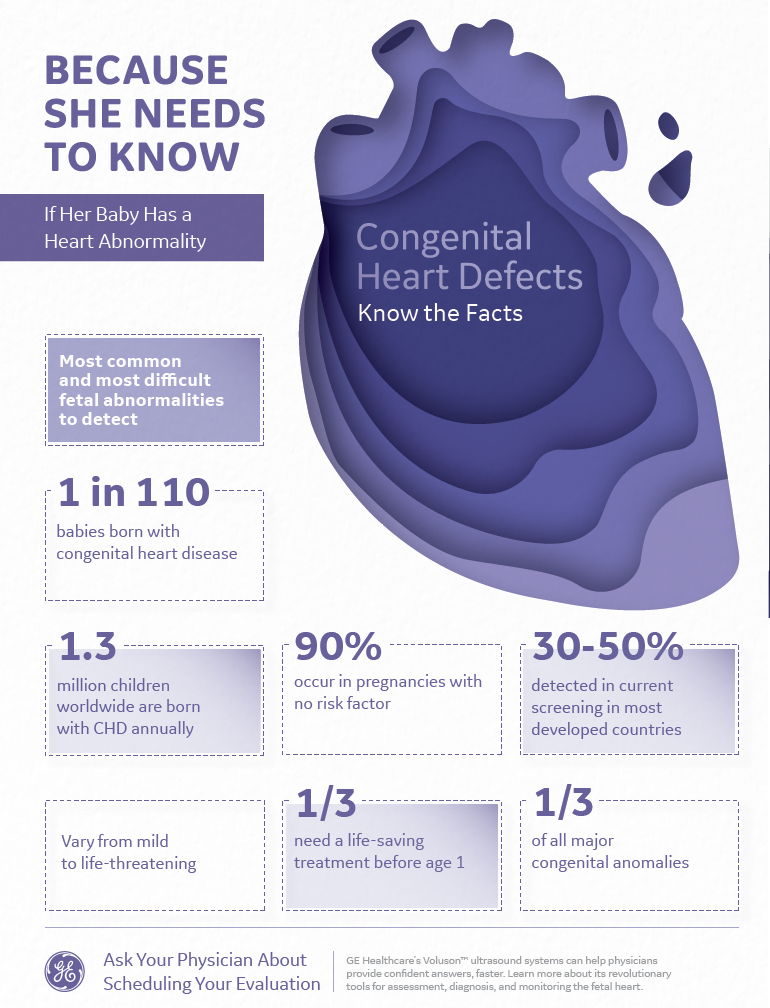
Learn about how ultrasound technologies can detect CHD here.
TOF is actually a set of four heart conditions occurring together:
- Ventricular Septal Defect: A hole between the heart's two lower ventricles.
- Pulmonary Stenosis: A narrowing that affects the pulmonary valve and main pulmonary artery.
- Overriding Aorta: The aortic valve is located above the ventricular septal defect.
- Ventricular Hypertrophy: A thickening of the right ventricle.
Although the cause of TOF is unknown, it is sometimes associated with other syndromic conditions such as Down and DiGeorge syndromes.
Identifying Tetralogy of Fallot Signs and Symptoms
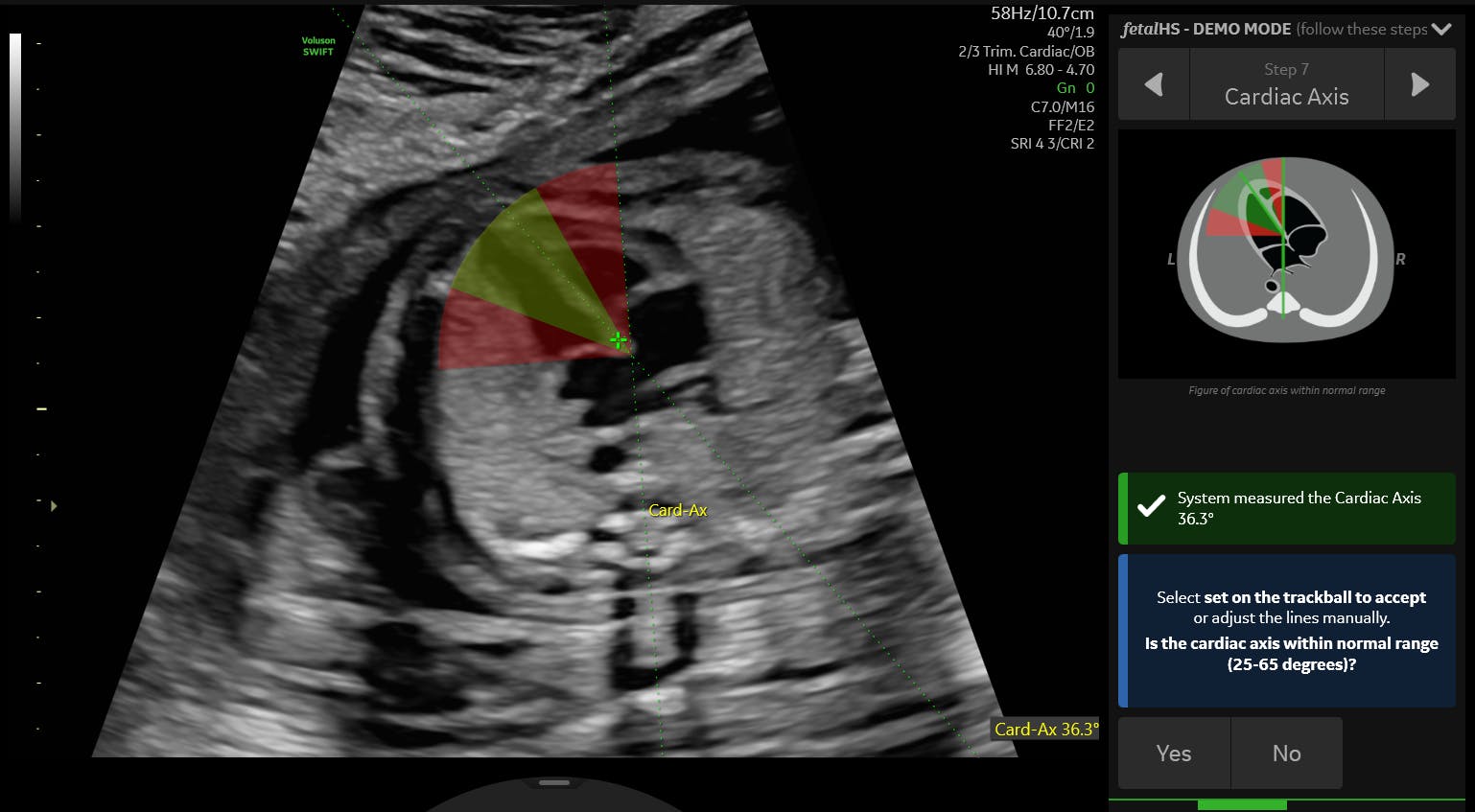
While clinician may be able to view a major heart defect such as TOF "as early as 10 weeks," per Ultrasound in Obstetrics & Gynecology, a four-chamber view as well as cardiac outflows can appear on ultrasound as early as eight weeks. However, these images are difficult to procure. Experienced operators rely on 4D imaging and high-resolution transvaginal probes to identify problematic cardiac structures at this early stage. If they suspect TOF, the appropriate follow-up test is a fetal echocardiogram.
Multiple studies have shown that about half of congenital heart defects go unnoticed during prenatal ultrasound screenings; in these cases, the signs and symptoms of TOF may not be recognized until after birth. The CDC writes that TOF is typically noticed shortly after birth, when infants may take on a bluish appearance while crying or feeding. These episodes of cyanosis are called 'tet spells.'
The Merck Manual describes 'tet spells' as hyper-cyanotic events that occur between birth and two years of age but seem to be most common between two and four months. These potentially deadly spells can stem from several factors but are usually the result of a decrease in oxygen saturation.
Routine pulse oximetry has been found useful in identifying asymptomatic newborns with this condition. In fact, the Journal of the American Medical Association (JAMA) published findings that routine screening with pulse oximetry for CCHDs reduced early infant deaths by more than 33 percent.
Diagnosing TOF and Developing a Treatment Plan
When possible, a prenatal diagnosis for TOF is preferable, since it gives the medical team advance notice for preparing a birth and neonatal care plan. Prenatal diagnosis is not always possible, but if confirmed, additional exams can point to the disease severity and the type of surgical repair likely to be required.
Cardiovascular Ultrasound reported useful parameters for evaluating TOF prenatally and predicting future care needs. Specifically, the pulmonary valve annulus z-score, the right PA (RPA) z-score, pulmonary valve peak systolic velocity, great artery annulus ratio and the RPA/descending aorta ratio performed during the second and third trimesters can help predict whether the infant is likely to require single- or multistage surgery.
The Merck Manual states that, although surgery for TOF is usually performed at two to six months of age, it may be performed earlier to address severe right ventricular outflow or if symptoms cannot otherwise be managed temporarily. If a complete repair is not possible due to factors such as low birth weight or complex anatomy, a shunt procedure may act as a temporary palliative measure.
Parents of infants whose surgical intervention will be delayed should receive education on caring for an infant with TOF. BJA Education describes interventions such as calming the child and placing the child in the knee-to-chest flexion position. Parents should also be educated on when to call for emergency services and undergo counselling on possible medications or supplemental oxygen needs.
Examining the Risks of Untreated TOF
Infants with TOF have a higher risk for certain conditions. The CDC lists these as endocarditis (an infection of the heart), arrhythmia, dizziness, fainting, seizures and growth or developmental delays. Additionally, infants released from the hospital undiagnosed with TOF face an increased risk of death.
The Merck Manual states that the perioperative mortality rate for patients with uncomplicated TOF is less than five percent. Untreated, the mortality rate is much higher; only about 55 percent of these patients will survive to reach five years of age, and just 30 percent will survive to age 10. The American Heart Association characterizes the long-term outlook for children with surgically-repaired TOF as "good" but still stresses the need for lifelong follow-up with a specially trained cardiologist. Some adults whose TOF was treated in childhood will require medication, additional surgeries, or pacemakers to address recurring concerns
In addition to medical concerns, families of children with this condition may face higher levels of stress and anxiety. BMJ Case Reports describes the experience of caring for a child with a CCHD as being fraught with a plethora of clinic visits from the time of prenatal diagnosis onward — and these visits are filled with medical terminology that may make it difficult to understand what's happening in their body. Additionally, these visits can cause financial pressure for parents and guardians due to travel, missed days of work and the cost of care. It is imperative to integrate emotional support for both children and their parents into patients' care plans.
Improving Outcomes With Early Diagnosis
Although the survivability of CCHDs has improved, it will take deeper understanding of the condition's etiology, diagnosis and treatment to further improve the tetralogy of Fallot prognosis.
Early diagnosis is important for effective management, but a complete understanding of the patient's condition is tantamount to determining the timing and type of surgical intervention needed to give each of these patients the best chance at a long, healthy life.