

Endometrial hyperplasia is characterized by hyperplastic changes in the glandular and stromal structures of the endometrium. It is one of the most frequent causes of abnormal uterine bleeding, which can lead to endometrial carcinoma if left untreated.
Atypical endometrial hyperplasia results from high levels of estrogen, combined with insufficient levels of progesterone. It is typically linked to postmenopausal women with unbalanced estrogen therapy, tamoxifen treatment, polycystic ovarian syndrome or obesity. Learning how to recognize and diagnose this condition according to the latest clinical recommendations can help you lead your patients to appropriate treatment as quickly as possible.
Improved Classification of Endometrial Hyperplasia
In 2014, the World Health Organization (WHO) simplified its classification system for the condition from four to two categories, replacing previous classification categories that often overlapped and led to improper diagnosis and treatment of hyperplasia, such as unnecessary hysterectomies.
Hyperplasia of the endometrium is now scored as either:
- Hyperplasia without atypia
- Atypical endometrial hyperplasia (endometrioid intraepithelial neoplasia)
The simplification into these two categories is due, in part, to a new understanding of the molecular genetic changes that occur with the condition, according to Geburtshilfe und Fraunheilekunde.
Hyperplasia without atypia exhibits only benign changes, which will return to normal when the abnormal gestagen levels that caused the condition have normalized. If an endocrine disorder caused these changes and persists in the long term, around 1 to 3 percent of those cases may progress to an invasive form. Atypical endometrial hyperplasia, on the other hand, contains many of the mutations seen in invasive endometrioid cancer; up to 60 percent of cases have a coexisting invasive cancer or a high risk of cancer.
Reducing Patient Risk Through Efficient Diagnosis
The two-part categorization allows for more effective diagnosis and treatment of endometrial hyperplasia. Hyperplasia without atypia can be treated conservatively by normalizing the cycle, prescribing oral contraceptives or hormonal IUDs and encouraging weight loss if necessary.
A hysterectomy, while not necessary to treat typical hyperplasia, can be considered in some cases, such as extreme obesity with no possibility of weight loss. The atypical hyperplasia uterus condition, alternatively, should be treated with a total hysterectomy. Conservative treatment using hormones with close monitoring is a route to consider if the patient wants to become pregnant in the future.
IETA Protocol for Endometrial Assessment
For appropriate assessment of endometrial hyperplasia during transvaginal ultrasound, the International Endometrial Tumor Analysis group (IETA) guidelines suggest measuring endometrial thickness in the sagittal plane, at the thickest portion perpendicular to the endometrial midline that includes the anterior and posterior endometrial layers.
This endometrial measurement must be done while viewing an appropriately magnified image and reported in millimeters, rounded up to one decimal point. The thickness of the endometrium should not include any fluid. If intracavitary fluid is present, the thickness of both single layers is measured and added together for a total reported sum.
An endometrial thickness of 4 mm or more in a postmenopausal woman with bleeding indicates a high risk of endometrial carcinoma. However, a biopsy may be necessary to exclude benign pathology that can cause bleeding and the appearance of hyperplasias, such as polyps or submucosal fibroids.
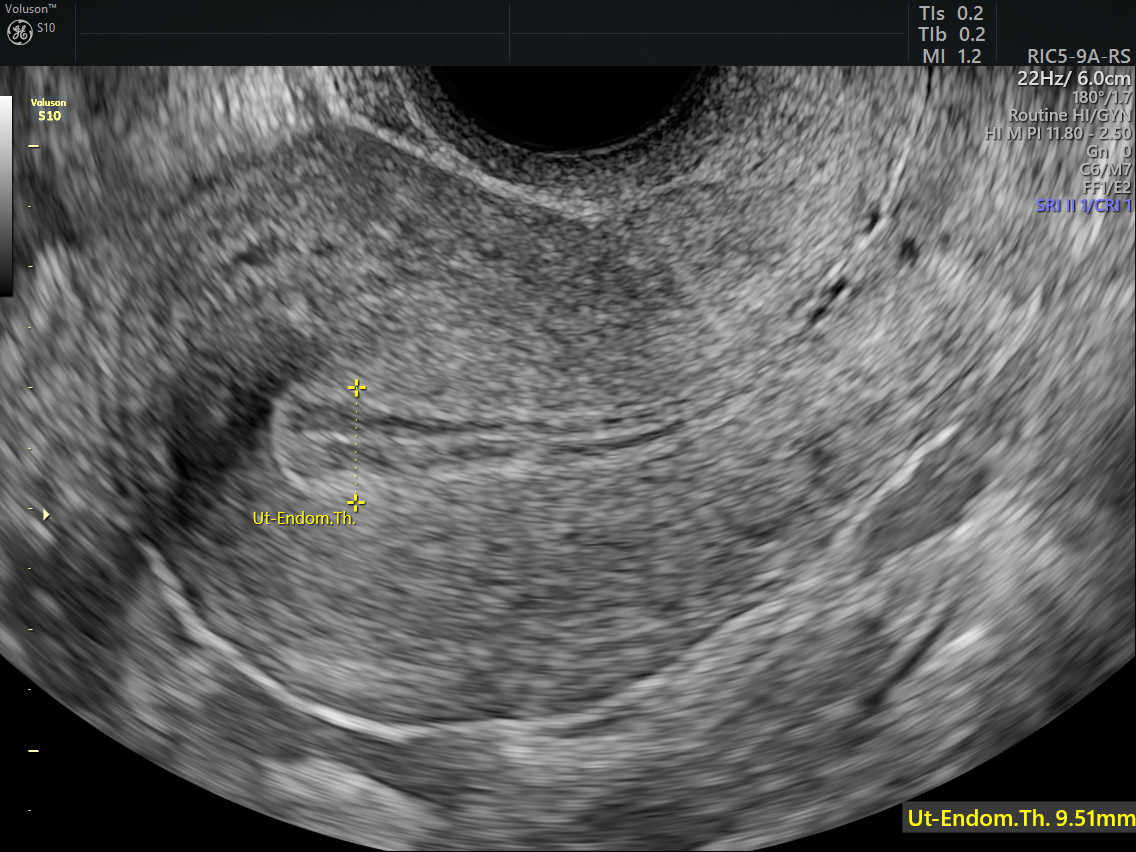
Measuring the Endometrium in 2D
2D Ultrasound of Thickened Endometrium
Making a Diagnosis With Ultrasound
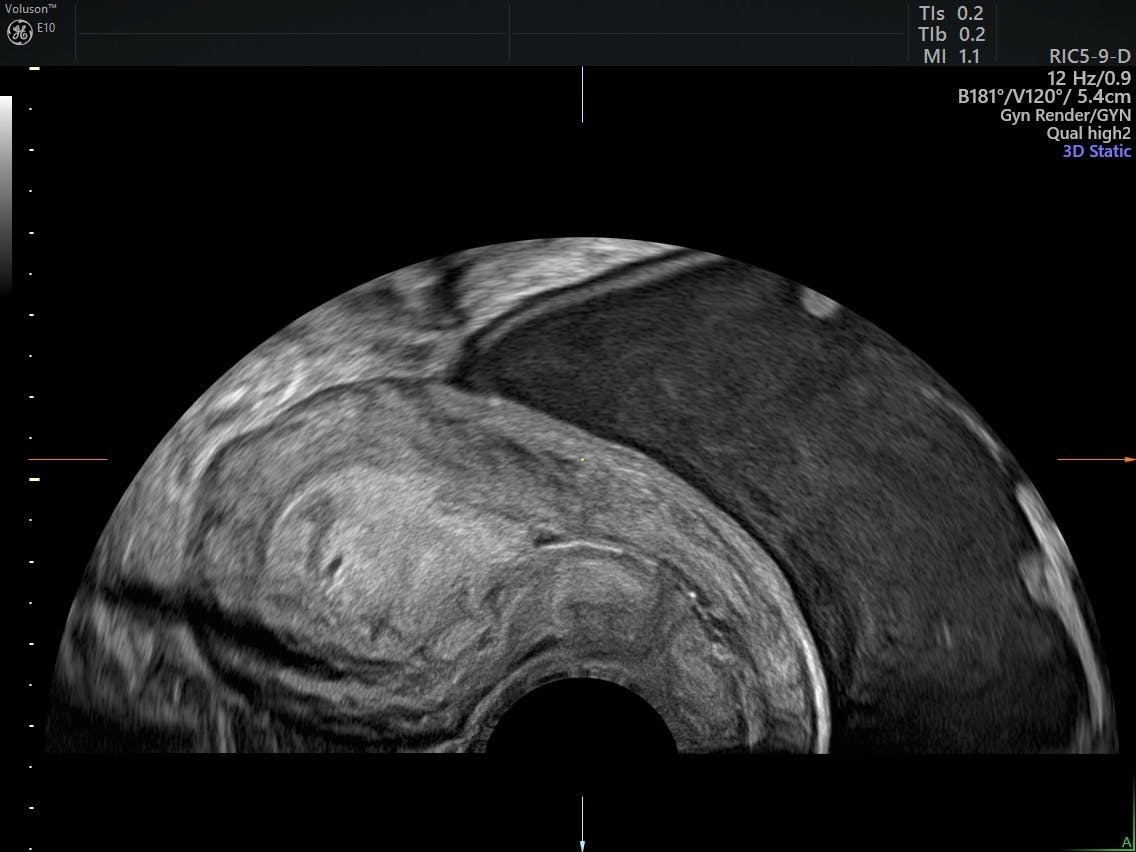
Transvaginal ultrasound is critical for assessing the endometrium and determining whether it appears homogeneous or nonhomogeneous, uniform or nonuniform. When used in conjunction with saline or gel infusion sonography, ultrasound can definitively identify polyps or fibroids within the endometrial canal.
Ultrasound can also help differentiate low- and high-risk endometrial cancers through various grayscale and color Doppler sonographic features. Ultrasound in Obstetrics and Gynaecology reports that high-risk tumors are more likely to have nonuniform echogenicity and an irregular endometrial-myometrial junction; contain a multiple, multifocal vessel pattern; and show a moderate to high color score.
Saline or gel infusion sonography is a helpful adjunct when the endometrium cannot be clearly visualized by transvaginal scanning alone. Fluid infusion can reveal benign pathology or help evaluate the morphology of a thickened endometrium.
The WHO's updated and simplified classification system is helping reduce the number of misdiagnoses of atypical endometrial hyperplasia. With the appropriate use of transvaginal ultrasound, sonohysterography and biopsy, clinicians are able to better assess and understand this condition and ultimately give patients the right care at the right time.



