
One hotly debated topic among fertility patients and the reproductive medicine community at large is whether a fresh or frozen embryo transfer results in more live births. In vitro fertilization (IVF) providers should familiarize themselves with the current research and statistics surrounding embryo transfers and learn how each method impacts the IVF process for patients and clinicians.
First Steps: The Priming Phase
Although there are many different approaches, fresh embryo transfers generally begin with a priming phase to suppress the patient's natural hormone production and ensure each follicle has the same likelihood of maturing.
Once the patient has a menstrual period, a baseline appointment checks for "quiet" ovaries via transvaginal ultrasound. Then, the ovarian stimulation phase begins. The goal is to produce as many mature eggs as possible — monitored via transvaginal ultrasound — without overstimulating the patient.
3D ultrasound tools like SonoAVC follicle automatically calculate the number and volume of stimulated follicles. This allows a gynecologist to monitor stimulation and pinpoint the optimal time for retrieval.
'We need to have precise measurements, so we can interrupt stimulation at the right time. More important than the number of follicles is the size. If a follicle is smaller than what you measured, you cannot use the egg to be fertilized. On the other hand, if it becomes too big, the egg might not be suitable for fertilization," says Dr. Angela Palumbo, director of the Centro de Fecundación In Vitro FIVAP.
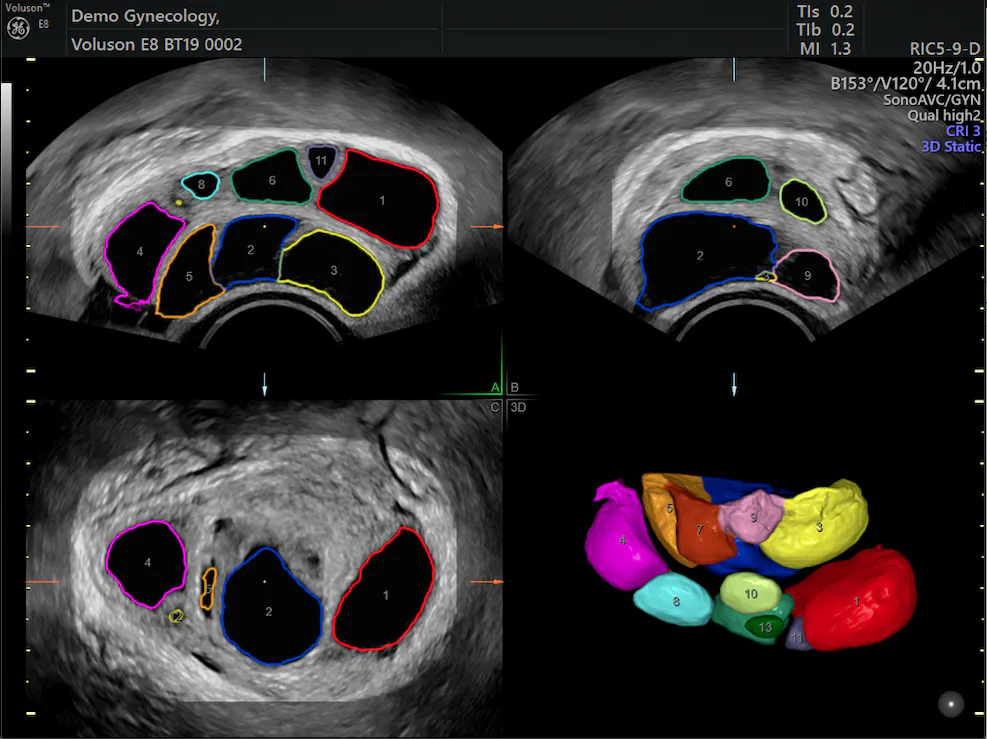
Stimulated follicles analyzed with SonoAVCfollicle
FIVAP providers use Voluson's SonoAVCfollicle to reduce potential errors in follicle counts. This tool allows a provider tosimply select an ovary and scan, removing the need for a manual count in most cases.
"It's a better way," Palumbo says, that may increase patients' chances of a healthy pregnancy. "We get more good follicles with mature eggs—which is what we want. That improves the IVF result."
Fresh Embryo Transfers
After seven to 14 days of stimulation, the patient takes a trigger injection at a specific time to help the eggs reach final maturation. Approximately 36 hours later, the reproductive endocrinologist retrieves the eggs and an embryologist attempts to fertilize them with sperm, either naturally or via intracytoplasmic sperm injection (ICSI).
Most fresh embryo transfers take place under ultrasound guidance at the blastocyst stage, five days after the egg retrieval. However, if the embryos do not develop well in the lab, the transfer may take place three days later instead. Any embryos not transferred are cryopreserved.
Live birth rates (LBR) following a fresh embryo transfer depend partly on patient age. According to the Society for Assisted Reproductive Technology (SART)'s 2016 report, the LBR was 36.7 percent for women under 35, 26.6 percent for women 35-37, 15.6 percent for women 38-40, and 9.3 percent for women 41 and older.
Frozen Embryo Transfers
A frozen transfer is much simpler for both the patient and reproductive endocrinologist. Just as with fresh embryos, the patient usually begins with the priming phase, followed by a baseline appointment.
The patient is typically prescribed some form of estradiol to develop the uterine lining, which is monitored via transvaginal ultrasound until it ideally reaches the 8- to 10-mm range and has a multilayer appearance.
Once that thickness is achieved, the reproductive endocrinologist directs the patient to begin taking progesterone to mimic the luteal phase. The provider schedules the frozen embryo transfer based on endometrial receptivity assay (ERA) results or on when the embryo was frozen. The embryo is then placed in the patient's uterus using ultrasound guidance.
SART found that LBRs for frozen eggs were 46.5 percent for women under 35, 38.6 percent for women 35-37, 29.4 percent for women 38-40, and 25.9 percent for women 41 and older — all significantly higher than fresh embryo transfers.
Fresh vs. Frozen Embryo Transfer: Other Considerations
A study published in Fertility and Sterility found that a woman's age is not the only determining factor when it comes to a live birth following an embryo transfer. High responders to ovarian stimulation had a 52 percent LBR in frozen embryo cycles compared to 48.9 percent in fresh embryo cycles. However, intermediate and low responders had a higher birth rate during fresh embryo cycles versus frozen embryo cycles (41.2 percent compared to 35.3 percent and 25.9 percent compared to 11.5 percent, respectively).
Another smaller study published in The New England Journal of Medicine found fresh transfers in ovulatory women had a higher live birth rate at 50.2 percent compared to 48.7 percent for frozen transfers, but the difference was not significant.
So what's the answer to the fresh-or-frozen question? It depends. Reproductive endocrinologists should take factors like age, stimulation response and ovulatory versus anovulatory status into account to make the recommendation that's best for each patient.



