

If you're confused about uterine anomalies, their classifications systems and their clinical relevance, or if you're struggling to remember the difference between a septate and arcuate uterus, or whether an anomaly is a single or combined variation, it's ok, you are not alone.
You can simplify and streamline the process of diagnosing abnormal uterus ultrasound results by following the steps below and documenting each patient's unique anatomic situation with the aid of your 3D ultrasound. The key is to describe what you see and to remember that the classification systems are simply frameworks. Every anomaly may not fit neatly into one category.
Best Practices for Categorizing Anomalies
I approach uterine anomalies by grouping them into one of three general categories:
- Failure to form
- Failure to fuse
- Failure to resorb or canalize
Embryology teaches us that two paramesonephric, or Müllerian, ducts form the female reproductive system by 20 weeks gestation. This includes development of the upper vagina, cervix, uterus and fallopian tubes. It coincides with the mesonephric, or Wolffian, duct development. Anomalies related to the development of the kidneys, ureters and bladder might also occur if there is a disturbance of the Müllerian ducts.
Uterine anomalies may be identified when these other associated anomalies, such as renal agenesis or ectopic kidney, are noted on a fetal anatomy scan or, more typically, much later after puberty. Since the ovaries function normally, the external genitalia are usually age-appropriate. Because many women are asymptomatic, the true incidence of uterine anomalies is not well understood.
Using 3D Ultrasound To Diagnose Uterine Anomalies
A woman's symptoms can vary from negligible to severe. She may present with no concerns or minor difficulties, such as being unable to use tampons. There may also be complaints of excruciating menses, the discovery of a pelvic mass or obstetric issues, such as recurrent pregnancy loss, preterm delivery or fetal malpresentation. You then consider a list of possible diagnoses in your mind, including uterine malformation.
Your first choice in imaging should be one of the following ultrasound exams:
- Transvaginal ultrasound
- Transabdominal ultrasound
- Saline infusion sonography (SIS) or saline contrast sonohysterography (SCSH)
Start by evaluating the entire pelvis carefully. If the patient is virginal, a transperineal or transabdominal ultrasound is best. Otherwise, perform a traditional, full transvaginal ultrasound. Check the position and size of the uterus, note its orientation and use 3D ultrasound to evaluate the contour and cavity.
Then examine at the cervix. Sweep from right to left to look for any additional structures, such as a uterine horn or pelvic kidney. You should also conduct a transabdominal scan to evaluate the position and presence of the kidneys. The patient's anatomy will steadily become discernible throughout this process.
Classifying Anomalies Based on the ASRM System
For classifying the anomaly, I prefer the 2016 American Society of Reproductive Medicine (ASRM) classification system. The European Society of Human Reproduction and Embryology (ESHRE) and European Society for Gynaecological Endoscopy (ESGE) classification system, which classifies the abnormalities of the uterus, cervix and vagina separately, is more difficult to apply in clinical practice.
The ASRM classification system describes general abnormalities from complete lack of development (Type I) and partial development (Type II) to fusion-related anomalies (Type III and IV) and failure of resorption (Type V and VI).
- Failure to form: If a uterus cannot be identified or appears hypoplastic, it would be considered a Type 1 anomaly, per the 2016 ASRM classification system. If only one horn is identified, this might well be a unicornuate (Type II) malformation where one of the paired Müllerian ducts has not developed.
- Failure to fuse: If both Müllerian ducts have developed but failed to fuse, two horns are present, as are two cervixes and often two vaginas. This would be a Type III lesion, or uterine didelphys. However, if the fusion only occurred lower in the genital tract but not more cephalad, the uterus appears heart shaped with two cavities — a Type IV, or bicornuate, uterus.
- Failure to resorb: Failure to resorb the tissue that has fused between the two Müllerian ducts results in a septate uterus with a divided cavity, a Type V defect. Resorption of all but the most fundal fused tissue results in a Type VI, or arcuate, uterus. Many feel an arcuate uterus is a variant of normal with no clinical impact. The differentiation of septate from arcuate has been arbitrarily defined as the existence of less than 1 cm of tissue indenting the cavity and protruding at an obtuse angle.
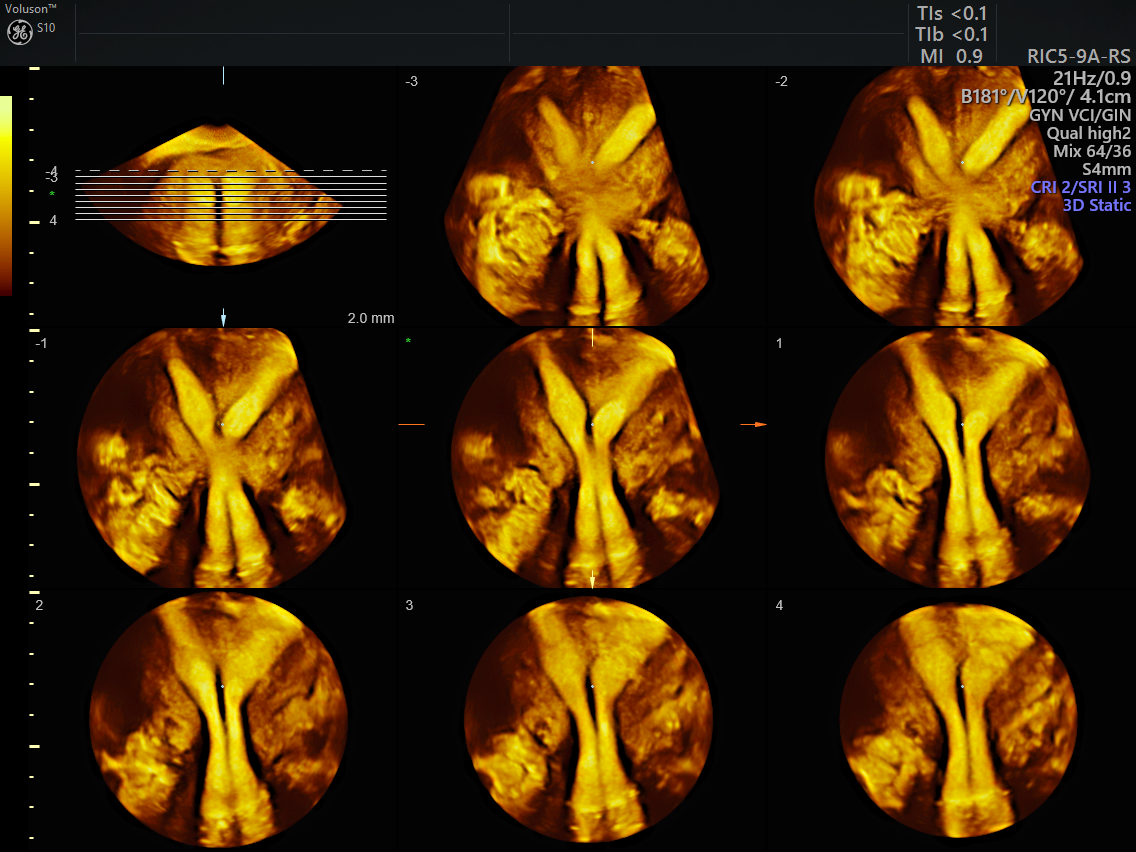
Completing the Exam With VCI and TUI
To complete the evaluation, consider performing an SIS or SCSH exam. This aids in delineating the cavity or cavities. If two cervixes are present, I typically conduct two separate SIS procedures using 3D ultrasound. A cineloop and careful labeling of your images is helpful for documentation and future review. This is also an ideal time to use volume contrast imaging (VCI) and tomographic ultrasound imaging (TUI) to better determine the anomaly.
VCI technology, which has been around for more than a decade, delivers improved visualization of organs and tissue margins. This is particularly helpful with tricky questions regarding anatomy. TUI displays many 2D slices from any volume of the three orthogonal planes, much like slices of a CT scan.
Uterine anomalies are challenging, even for the most experienced clinicians. The secret is to simply describe what you see and to be patient. A planned, careful, stepwise evaluation with full use of your ultrasound will give you the satisfaction of unraveling this Gordian knot.
Abnormal uterus ultrasound



