
The female infertility workup has changed dramatically over the past few decades. From low-cost, noninvasive ultrasounds to laparoscopic surgery, reproductive endocrinologists now have many tools at their disposal.
For each infertility test, patients must understand the step-by-step process of how the procedure is performed, any pain they might expect, what defines normal and abnormal results, how their results fall into these ranges and what abnormal results mean for their overall fertility. Informed patients can make better decisions about their own care when it comes to navigating infertility.
We've provided an overview of each test and how to explain it to patients.
Blood Hormone Levels
Reproductive endocrinologists should start any new patient evaluation with a conversation about the female reproductive system. Many women don't understand the roles their hormones and reproductive organs play in the intricate conception process.
Because the couple's inability to conceive may hinge on the female partner's hormones, her blood should be drawn early in her menstrual cycle — typically between days two and four — to check AMH, E2, FSH, LH, P4, free testosterone and total testosterone levels.
Other levels that may prove helpful in her diagnosis include DHEA-S, vitamin D, T3, T4, TSH, prolactin and any other tests indicated by the patient's history.
Transvaginal Ultrasound
No female infertility workup is complete without a transvaginal ultrasound.
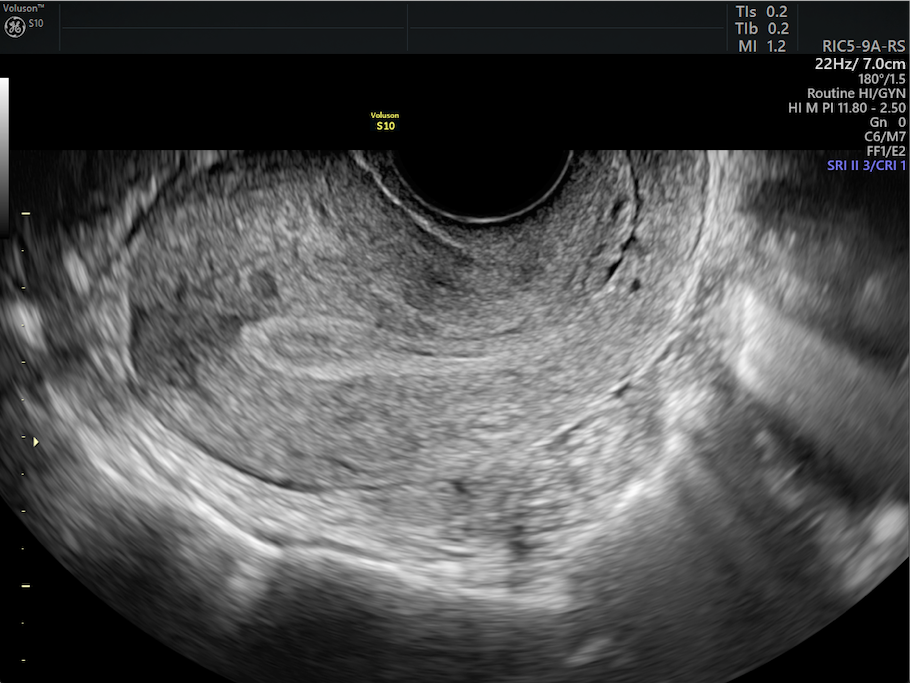
Transvaginal ultrasound image of uterus and endometrium.
Reproductive endocrinologists should explain that despite being inserted into the vagina, this procedure is routine, painless and non-ionizing. Patients should be offered the opportunity to place the ultrasound camera (known as a transducer or probe) themselves, if doing so would further increase their comfort.
The sonographer or physician should describe what the patient is seeing on the monitor, including an antral follicle count, follicle sizes, endometrium thickness and any abnormalities. If the clinic has a 3D ultrasound machine, the technician can evaluate planes of the uterus not available with 2D, allowing the diagnosis of any congenital uterine malformations.
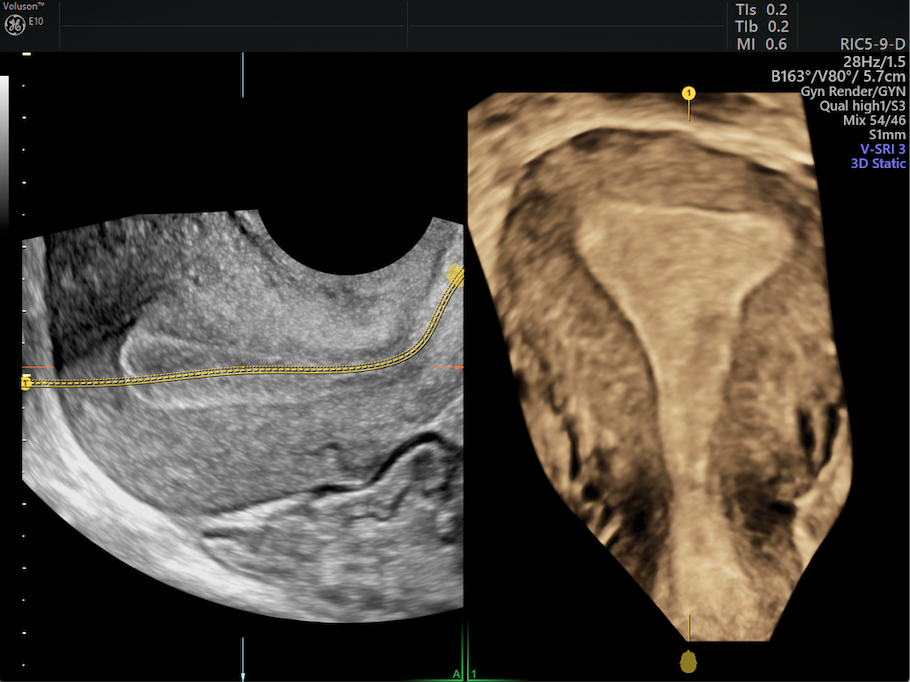
3D ultrasound volume showing a normal shape. This shape cannot be seen with 2D imaging alone.

Uterus with common malformation of a partial septum through the center of the uterine cavity.
Sonohysterogram (SHG) or Saline-Infused Sonography (SIS)
Because the SHG/SIS — especially when combined with a sonosalpingogram — allows reproductive endocrinologists to further evaluate a patient's uterine structure and lining and also check her fallopian tubes for blockages, physicians should explain the value of including this type of ultrasound in the initial infertility workup.
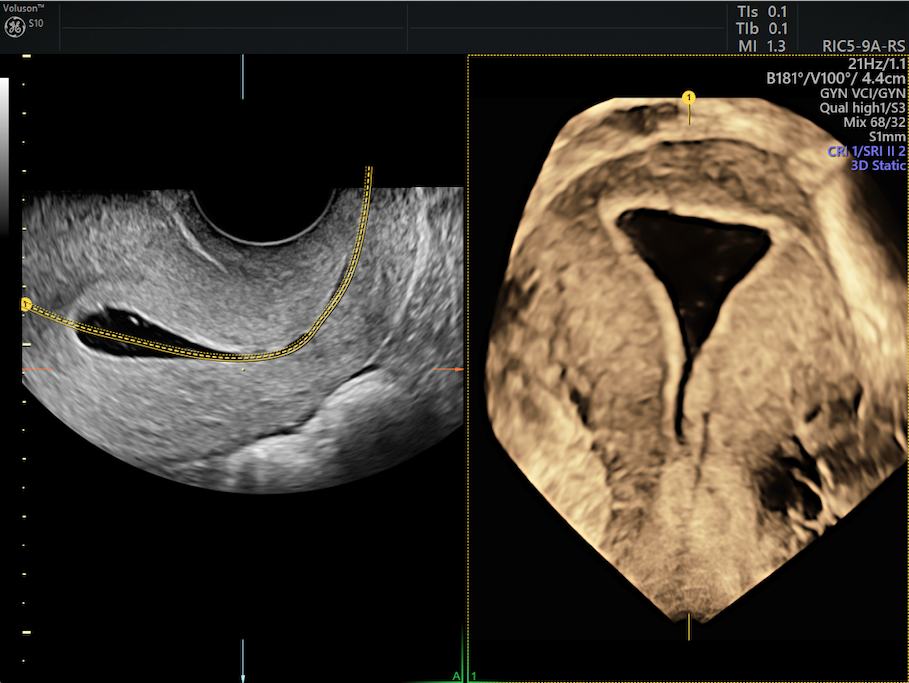
Saline infusion allows the cavity to be distended and visualize the contour of the cavity.
Patients should be made aware that they will need to have it scheduled after their period ends but before they ovulate. As far as the procedure itself, doctors should walk them through step by step, including the role ultrasound plays and how they might experience some pain from the liquid being pushed into their uterus and tubes.
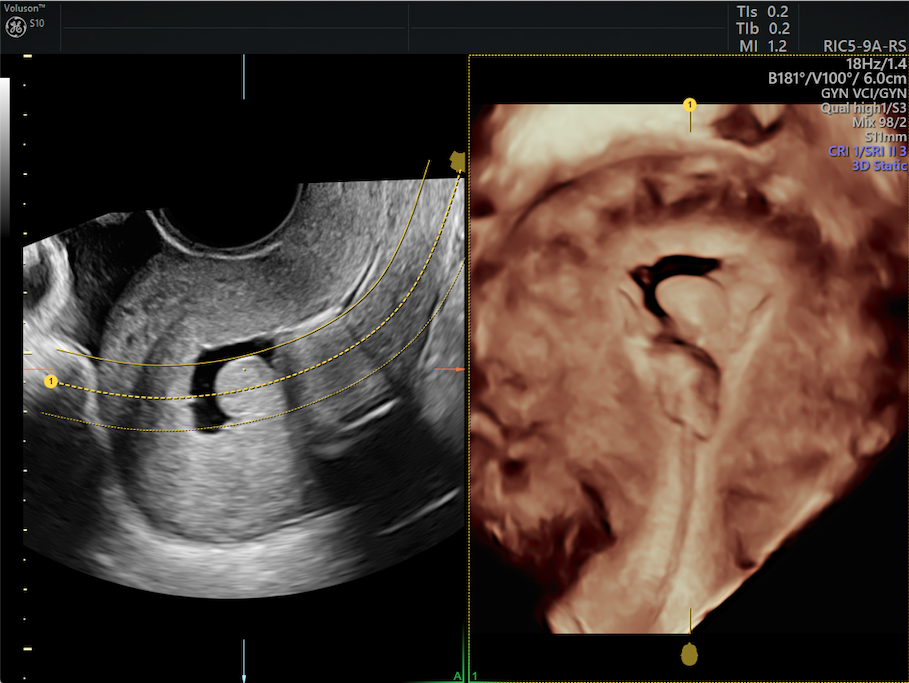
3D Ultrasound image after saline infusion showing a polyp in the endometrium.
Hysterosalpingogram (HSG)
Most women undergoing an infertility workup are at least somewhat familiar with the HSG. Although many reproductive endocrinologists now favor the SHG/SIS over the HSG, if this procedure is recommended, patients are likely to be nervous and might benefit from pre-medicating with over-the-counter or prescription pain medication.
Like the SHG/SIS, patients should schedule this procedure after their period ends but before they ovulate. Because X-ray and contrast dye are used instead of ultrasound to evaluate patients' uterus for abnormalities and fallopian tubes for blockages, physicians should discuss the risks involved as well as the procedure itself.
Because pain tolerance varies person to person, doctors should be empathetic of any pain their patients experience as a result of the HSG. Reproductive endocrinologists should reassure patients that the HSG provided valuable insight, either ruling out or confirming specific diagnoses.
Hysteroscopy and Laparoscopy
If uterine abnormalities are suspected and perhaps in need of correction, a hysteroscopy or laparoscopy might be warranted. Because these are surgical procedures, patients should be made aware of the risks and possible complications.
Although much more invasive than the other diagnostic methods already described in this article, reproductive endocrinologists should comfort patients with the fact that hysteroscopies are generally considered safe and can be performed right at the fertility clinic under light sedation. For those wondering when to do laparoscopy for infertility, this procedure — which is performed in an operating room — is a better option if endometriosis, pelvic inflammatory disease, pelvic adhesions or hydrosalpinx are suspected. Either way, physicians should explain what to expect and calm any nerves.
Once patients are fully awake, doctors should describe how the procedure went and anything of note that was discovered or addressed. Patients should also leave with a list of all warning signs that warrant a call to the office or after-hours emergency line.
While all of these procedures may seem intimidating to patients at first, keeping patients informed throughout the process should help ease their concerns, thereby leading to more positive outcomes.



